Adenoma hipofisário silencioso é um tumor benigno da hipófise que não produz hormônios em excesso, sendo frequentemente descoberto incidentalmente. Pode causar sintomas por compressão de estruturas vizinhas ou, raramente, por deficiência hormonal.
Introdução
O que você precisa saber de cara
Visão geral
O adenoma hipofisário silencioso é um tumor benigno (não canceroso) que se forma na glândula hipófise, localizada na base do cérebro. Diferentemente de outros adenomas hipofisários, ele não produz hormônios em quantidade suficiente para causar sintomas hormonais clássicos, sendo chamado de 'silencioso'. A doença é considerada rara e, no Brasil, não possui cobertura específica pelo Sistema Único de Saúde (SUS).[1]
Sinais e sintomas
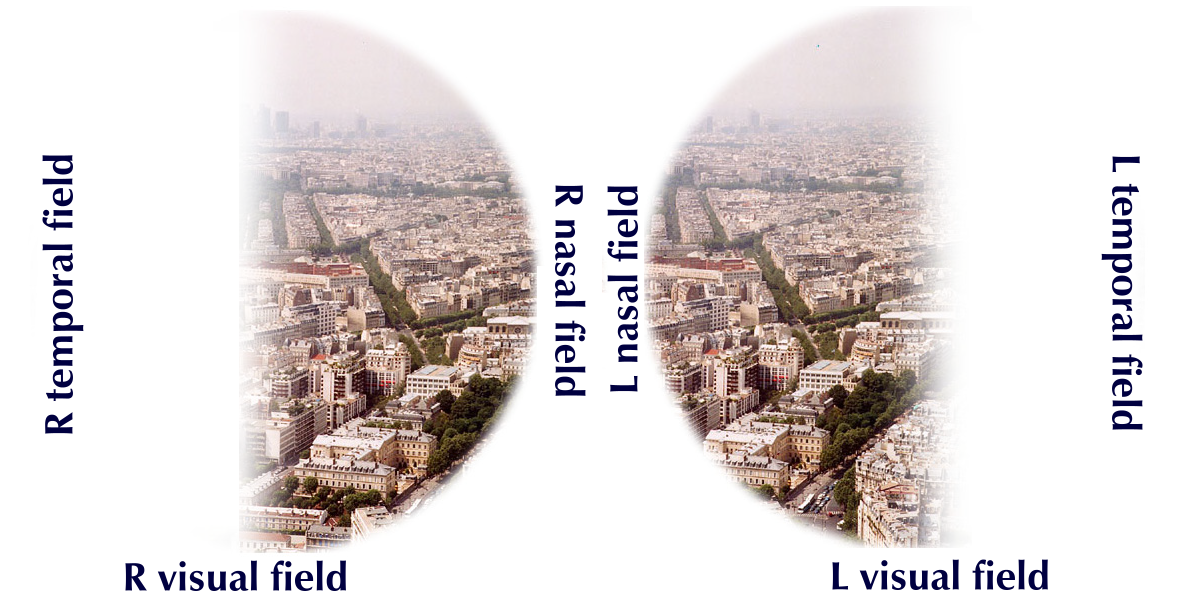
Por ser um tumor que não secreta hormônios em excesso, os sintomas geralmente surgem devido ao crescimento do tumor e à compressão de estruturas vizinhas, como o nervo óptico. Os principais sinais incluem dores de cabeça persistentes, alterações na visão (como perda de campo visual) e, em alguns casos, alterações no funcionamento da hipófise que podem levar a desequilíbrios hormonais leves. No entanto, muitos pacientes podem não apresentar sintomas por longos períodos.[1]
Causas genéticas
A causa exata do adenoma hipofisário silencioso não é completamente compreendida, mas alterações genéticas estão envolvidas. Mutações nos genes MEN1 (que produz a proteína menina) e AIP (que produz uma proteína ribossômica) foram associadas ao desenvolvimento desse tipo de tumor. Esses genes são conhecidos por estarem relacionados a síndromes genéticas que aumentam o risco de tumores hipofisários.[1][3]
Diagnóstico
O diagnóstico é baseado em exames de imagem, como ressonância magnética da hipófise, que identifica a presença do tumor. Exames de sangue para dosagem hormonal ajudam a confirmar que o tumor não está produzindo hormônios em excesso. Testes genéticos podem ser realizados para identificar mutações nos genes MEN1 e AIP, e estão disponíveis em laboratórios especializados (mais de 330 testes genéticos listados em bases internacionais). Atualmente, mais de 1.000 variantes genéticas associadas à doença estão catalogadas no ClinVar.[1][3]
Tratamento e manejo
O tratamento depende do tamanho do tumor, dos sintomas e da presença de complicações. As opções incluem cirurgia para remoção do tumor (especialmente se houver compressão do nervo óptico), radioterapia e, em alguns casos, acompanhamento clínico com exames periódicos. Não há medicamentos específicos aprovados para o adenoma hipofisário silencioso, e o manejo é individualizado, com base na avaliação de um endocrinologista e neurocirurgião. No Brasil, o tratamento não é coberto pelo SUS para esta condição específica.[1]
Tratamentos citados na literatura
Não há fármacos listados na literatura científica como tratamentos específicos para o adenoma hipofisário silencioso. Portanto, esta seção não contém informações adicionais.[1]
Prognóstico e qualidade de vida
O prognóstico geralmente é bom, pois o tumor é benigno e de crescimento lento. Com o tratamento adequado, a maioria dos pacientes tem uma boa qualidade de vida. No entanto, complicações como perda de visão podem ser irreversíveis se não tratadas precocemente. O acompanhamento regular com exames de imagem e hormonais é importante para monitorar o crescimento do tumor e ajustar o tratamento conforme necessário.[1]
Conteúdo informativo gerado e mantido automaticamente a partir de fontes oficiais (Orphanet, HPO, OMIM, SUS). Não substitui avaliação médica.
Adenoma hipofisário silencioso é um tumor benigno da hipófise que não produz hormônios em excesso, sendo frequentemente descoberto incidentalmente. Pode causar sintomas por compressão de estruturas vizinhas ou, raramente, por deficiência hormonal.
Encontrou um erro ou informação desatualizada? Sugira uma correção →
Entender a doença
Do básico ao detalhe, leia no seu ritmo
Preparando trilha educativa...
Sinais e sintomas
O que aparece no corpo e com que frequência cada sintoma acontece
Visão geral
O adenoma hipofisário silencioso é um tumor benigno (não canceroso) que se forma na glândula hipófise, localizada na base do cérebro. Diferentemente de outros adenomas hipofisários, ele não produz hormônios em quantidade suficiente para causar sintomas hormonais clássicos, sendo chamado de 'silencioso'. A doença é considerada rara e, no Brasil, não possui cobertura específica pelo Sistema Único de Saúde (SUS).[1]
Sinais e sintomas
Por ser um tumor que não secreta hormônios em excesso, os sintomas geralmente surgem devido ao crescimento do tumor e à compressão de estruturas vizinhas, como o nervo óptico. Os principais sinais incluem dores de cabeça persistentes, alterações na visão (como perda de campo visual) e, em alguns casos, alterações no funcionamento da hipófise que podem levar a desequilíbrios hormonais leves. No entanto, muitos pacientes podem não apresentar sintomas por longos períodos.[1]
Causas genéticas
A causa exata do adenoma hipofisário silencioso não é completamente compreendida, mas alterações genéticas estão envolvidas. Mutações nos genes MEN1 (que produz a proteína menina) e AIP (que produz uma proteína ribossômica) foram associadas ao desenvolvimento desse tipo de tumor. Esses genes são conhecidos por estarem relacionados a síndromes genéticas que aumentam o risco de tumores hipofisários.[1][3]
Diagnóstico
O diagnóstico é baseado em exames de imagem, como ressonância magnética da hipófise, que identifica a presença do tumor. Exames de sangue para dosagem hormonal ajudam a confirmar que o tumor não está produzindo hormônios em excesso. Testes genéticos podem ser realizados para identificar mutações nos genes MEN1 e AIP, e estão disponíveis em laboratórios especializados (mais de 330 testes genéticos listados em bases internacionais). Atualmente, mais de 1.000 variantes genéticas associadas à doença estão catalogadas no ClinVar.[1][3]
Tratamento e manejo
O tratamento depende do tamanho do tumor, dos sintomas e da presença de complicações. As opções incluem cirurgia para remoção do tumor (especialmente se houver compressão do nervo óptico), radioterapia e, em alguns casos, acompanhamento clínico com exames periódicos. Não há medicamentos específicos aprovados para o adenoma hipofisário silencioso, e o manejo é individualizado, com base na avaliação de um endocrinologista e neurocirurgião. No Brasil, o tratamento não é coberto pelo SUS para esta condição específica.[1]
Tratamentos citados na literatura
Não há fármacos listados na literatura científica como tratamentos específicos para o adenoma hipofisário silencioso. Portanto, esta seção não contém informações adicionais.[1]
Prognóstico e qualidade de vida
O prognóstico geralmente é bom, pois o tumor é benigno e de crescimento lento. Com o tratamento adequado, a maioria dos pacientes tem uma boa qualidade de vida. No entanto, complicações como perda de visão podem ser irreversíveis se não tratadas precocemente. O acompanhamento regular com exames de imagem e hormonais é importante para monitorar o crescimento do tumor e ajustar o tratamento conforme necessário.[1]
Conteúdo informativo gerado e mantido automaticamente a partir de fontes oficiais (Orphanet, HPO, OMIM, SUS). Não substitui avaliação médica.
Linha do tempo da pesquisa
Encontrou um erro ou informação desatualizada? Sugira uma correção →
Genética e causas
O que está alterado no DNA e como passa nas famílias
Genes associados
2 genes identificados com associação a esta condição.
Essential component of a MLL/SET1 histone methyltransferase (HMT) complex, a complex that specifically methylates 'Lys-4' of histone H3 (H3K4). Functions as a transcriptional regulator. Binds to the TERT promoter and represses telomerase expression. Plays a role in TGFB1-mediated inhibition of cell-proliferation, possibly regulating SMAD3 transcriptional activity. Represses JUND-mediated transcriptional activation on AP1 sites, as well as that mediated by NFKB subunit RELA. Positively regulates
Nucleus
Familial multiple endocrine neoplasia type I
Autosomal dominant disorder characterized by tumors of the parathyroid glands, gastro-intestinal endocrine tissue, the anterior pituitary and other tissues. Cutaneous lesions and nervous-tissue tumors can exist. Prognosis in MEN1 patients is related to hormonal hypersecretion by tumors, such as hypergastrinemia causing severe peptic ulcer disease (Zollinger-Ellison syndrome, ZES), primary hyperparathyroidism, and acute forms of hyperinsulinemia.
May act as a negative regulator of Aurora-A kinase, by down-regulation through proteasome-dependent degradation
Mitochondrion matrixNucleus
Variantes genéticas (ClinVar)
1.066 variantes patogênicas registradas no ClinVar.
Vias biológicas (Reactome)
11 vias biológicas associadas aos genes desta condição.
Diagnóstico
Os sinais que médicos procuram e os exames que confirmam
Tratamento e manejo
Remédios, cuidados de apoio e o que precisa acompanhar
Onde tratar no SUS
Hospitais de referência no Brasil e o protocolo oficial do SUS (PCDT)
🇧🇷 Atendimento SUS — Adenoma hipofisário silencioso
Selecione um estado ou use sua localização para ver resultados.
Dados de DATASUS/CNES, SBGM, ABNeuro e Ministério da Saúde. Sempre confirme a disponibilidade diretamente com o estabelecimento.
Pesquisa ativa
Ensaios clínicos abertos e novidades científicas recentes
Ensaios em destaque
🟢 Recrutando agora
3 pesquisas recrutando participantes. Converse com seu médico sobre a possibilidade de participar.
Outros ensaios clínicos
18 ensaios clínicos encontrados, 3 ativos.
Publicações mais relevantes
Association between Intracellular Calcium Signaling and Tumor Recurrence in Human Non-Functioning Pituitary Adenomas.
Clinically non-functioning pituitary adenomas (CNFPAs) are the second most frequent sellar tumor among studies on community-dwelling adults. They are characterized by the absence of hormonal hypersecretion syndrome, and patients present with compressive symptoms, such as a headache and visual field defects. Immunohistochemically, most CNFPAs are of gonadotrope differentiation, with only a few of them being truly null cell adenomas. Although these tumors express receptors for one or more hypothalamic releasing hormones, to what extent this has an impact on the biological and clinical behavior of these neoplasms remains to be defined. In this research, we evaluated the basal and hypothalamic secretagogue-stimulated intracellular calcium mobilization in 13 CNFPAs, trying to correlate this response to the phenotypic features of the patients. Our results indicate that the recurrence of a CNFPA correlates positively with cellular responsiveness, as measured by spontaneous intracellular calcium activity and the ability to respond to multiple hypothalamic secretagogues. We conclude that this finding may be a useful tool for predicting the clinicopathologic behavior of CNFPAs, by testing the variation of cellular responsiveness to hypothalamic secretagogues.
Phenotype Transformation of PitNETs.
Phenotype transformation in pituitary neuroendocrine tumors is a little-known and unpredictable clinical phenomenon. Previous studies have not clearly defined and systematically concluded on the causes of this rare phenomenon. Additionally, the mechanisms of phenotype transformation are not well known. We reviewed cases reported in the literature with the aim of defining phenotype transformation in pituitary neuroendocrine tumors. We present an overview of the wide spectrum of phenotype transformation and its clinical features. We also discuss findings on the potential mechanism of this rare transformation, which may be related to PC1/3, the bioactivity of secretory hormones, gene mutations and the plasticity of pituitary neuroendocrine tumors. Clinicians should be aware of this rare phenomenon and more studies on the underlying mechanisms are required.
Elevated risk of recurrence and retreatment for silent pituitary adenomas.
Pituitary adenomas are the most common tumor of the pituitary gland and comprise nearly 15% of all intracranial masses. These tumors are stratified into functional or silent categories based on their pattern of hormone expression and secretion. Preliminary evidence supports differential clinical outcomes between some functional pituitary adenoma (FPA) subtypes and silent pituitary adenoma (SPA) subtypes. We collected and analyzed the medical records of all patients undergoing resection of SPAs or FPAs from a single high-volume neurosurgeon between 2007 and 2018 at Brigham and Women's Hospital. Descriptive statistics and the Mantel-Cox log-rank test were used to identify differences in outcomes between these cohorts, and multivariate logistic regression was used to identify predictors of radiographic recurrence for SPAs. Our cohort included 88 SPAs and 200 FPAs. The majority of patients in both cohorts were female (48.9% of SPAs and 63.5% of FPAs). SPAs were larger in median diameter than FPAs (2.1 cm vs. 1.2 cm, p < 0.001). The most frequent subtypes of SPA were gonadotrophs (55.7%) and corticotrophs (30.7%). Gross total resection (GTR) was achieved in 70.1% of SPA resections and 86.0% of FPA resections (p < 0.001). SPAs had a higher likelihood of recurring (hazard ratio [HR] 3.2, 95% confidence interval [95%CI] 1.6-7.2) and a higher likelihood of requiring retreatment for recurrence (HR 2.5; 95%CI 1.0-6.1). Subset analyses revealed that recurrence and retreatment were more both likely for subtotally resected SPAs than subtotally resected FPAs, but this pattern was not observed in SPAs and FPAs after GTR. Among SPAs, recurrence was associated with STR (odds ratio [OR] 9.3; 95%CI 1.4-64.0) and younger age (OR 0.92 per year; 95%CI 0.88-0.98) in multivariable analysis. Of SPAs that recurred, 12 of 19 (63.2%) were retreated with repeat surgery (n = 11) or radiosurgery (n = 1), while the remainder were observed (n = 7).There were similar rates of recurrence across different SPA subtypes. Patients undergoing resection of SPAs should be closely monitored for disease recurrence through more frequent clinical follow-up and diagnostic imaging than other adenomas, particularly among patients with STR and younger patients. Several patients can be observed after radiographic recurrence, and the decision to retreat should be individualized. Longitudinal clinical follow-up of SPAs, including an assessment of symptoms, endocrine function, and imaging remains critical.
Nonfunctioning Pituitary Lesions.
Nonfunctioning pituitary lesions represent a subset of pituitary adenomas that do not manifest with clinical features of hormone hypersecretion. Because of their indolent nature, their diagnosis is elusive, often resulting in presentation after the tumors have grown large enough to cause compressive symptoms. Although they are clinically silent, the various subtypes correspond to the predominant cell line of origin and therefore are biochemically distinct from one another. This article reviews the biochemical, clinical, and histopathologic features of each of these subtypes. A rubric is provided for diagnostic work-up of these lesions and the management options available to the treating clinician.
Clinical Relevance and Immunohistochemical Patterns of Silent Pituitary Adenomas: 10 Years of Single-centre Experience.
Silent pituitary adenomas are clinically non-functional (i.e., without clinically evident pituitary hormone production). The aim of this study was to investigate subjects with silent pituitary adenomas for possible variations in their clinical status. A total of 102 patients who had undergone surgery for pituitary adenoma and had been diagnosed with silent pituitary adenoma was included in the study. The patients' preoperative and postoperative hormonal parameters and magnetic resonance imaging (MRI) features were collected, and pathological specimens were re-evaluated. Immunohistochemistry results of the 102 patients were as follows: hormone-negative adenomas (n=35) 35.5%; FSH+LH-positivity (n=32) 31.3%; ACTH-positivity (n=11) 10.7%; α-subunit- positivity (n= 9) 8.8%; prolactin-positivity (n=8) 7.8%; GH-positivity (n=6) 5.4%; and plurihormonal adenoma (n=1). The mean sizes of SGA, SGHA, and SCA were 28.0±12.7, 30.0±16.0, and 27.7±8.9mm (p>0.05), respectively. With the exception of silent gonadotroph adenomas (SGAs), female gender dominance was shown in patients with silent growth hormone adenoma (SGHA) and silent corticotroph adenoma (SCA). Although no clinical relevance was observed in relation to hormonal excess, preoperative GH (4.21±4.6, vs. 0.27±0.36 p=0.00) was slightly more elevated in SGHA than in GH-negative adenomas. Additionally, preoperative basal ACTH values (47.3±28.7 vs. 23.9±14.4, p=0.003) were also higher in SCA compared to the other types. Our findings revealed SCAs to be of more aggressive behaviour than SGHAs and SGAs due to invasiveness in radiological imaging, their elevated re-operation, and postoperative ACTH values. Silent pituitary adenomas represent a challenging diagnostic tumour group. Careful initial evaluation of patients with pituitary adenomas should consider any mild signs and symptoms of functionality, particularly in cases of GH- and ACTH-secreting adenomas.
Publicações recentes
[Endocrine inactive pituitary microadenomas: current data on natural history and follow-up approaches].
Oxidative Phosphorylation in Silent Pituitary Adenomas: A Multiomics Perspective.
Silent growth hormone pituitary adenomas: a single-center study.
Characteristics and treatment of a silent somatotroph tumor that had transformed to a functional type: a case report and literature review.
Suspected silent pituitary somatotroph neuroendocrine tumor associated with acromegaly-like bone disorders: a case report.
📚 EuropePMC7 artigos no totalmostrando 16
Phenotype Transformation of PitNETs.
CancersAssociation between Intracellular Calcium Signaling and Tumor Recurrence in Human Non-Functioning Pituitary Adenomas.
International journal of molecular sciencesElevated risk of recurrence and retreatment for silent pituitary adenomas.
PituitaryNonfunctioning Pituitary Lesions.
Otolaryngologic clinics of North AmericaClinical Relevance and Immunohistochemical Patterns of Silent Pituitary Adenomas: 10 Years of Single-centre Experience.
Current medical imagingSilent pituitary adenoma and metabolic disorders: obesity, abnormal glucose tolerance, hypertension and dyslipidemia.
Endocrine journalClinical characteristics and outcomes of null-cell versus silent gonadotroph adenomas in a series of 1166 pituitary adenomas from a single institution.
Neurosurgical focusMSH6/2 and PD-L1 Expressions Are Associated with Tumor Growth and Invasiveness in Silent Pituitary Adenoma Subtypes.
International journal of molecular sciencesFunction of cell-cycle regulators in predicting silent pituitary adenoma progression following surgical resection.
Oncology lettersAggressive somatotrophinomas lacking clinical symptoms: neurosurgical management.
Neurosurgical reviewGangliocytoma: outcome of a rare silent pituitary tumour.
BMJ case reportsBiological and radiological exploration and management of non-functioning pituitary adenoma.
Annales d'endocrinologiePost-surgical management of non-functioning pituitary adenoma.
Annales d'endocrinologieManagement of clinically non-functioning pituitary adenoma.
Annales d'endocrinologieNon-functioning pituitary adenoma: when and how to operate? What pathologic criteria for typing?
Annales d'endocrinologieSilent pituitary adenomas.
Endocrinology and metabolism clinics of North AmericaAssociações
Organizações que acompanham esta doença — pra ter apoio e orientação
Ainda não temos associações cadastradas para Adenoma hipofisário silencioso.
É de uma associação que acompanha esta doença? Fale com a gente →
Comunidades
Grupos ativos de quem convive com esta doença aqui no Raras
Ainda não existe comunidade no Raras para Adenoma hipofisário silencioso
Pacientes, familiares e cuidadores se organizam em comunidades pra compartilhar experiências, fazer perguntas e se apoiar. Você pode ser o primeiro.
Tire suas dúvidas
Perguntas, dicas e experiências compartilhadas aqui na página
Participe da discussão
Faça login para postar dúvidas, compartilhar experiências e interagir com especialistas.
Fazer loginDoenças relacionadas
Doenças com sintomas parecidos — ajudam quem ainda está buscando diagnóstico
Ainda não achamos doenças com sintomas parecidos o suficiente.
Referências e fontes
Bases de dados externas citadas neste artigo
Publicações científicas
Artigos indexados no PubMed ligados a esta doença no grafo RarasNet — título, periódico e PMID direto da fonte, sem intermediação de IA.
- Association between Intracellular Calcium Signaling and Tumor Recurrence in Human Non-Functioning Pituitary Adenomas.
- Phenotype Transformation of PitNETs.
- Elevated risk of recurrence and retreatment for silent pituitary adenomas.
- Nonfunctioning Pituitary Lesions.
- Clinical Relevance and Immunohistochemical Patterns of Silent Pituitary Adenomas: 10 Years of Single-centre Experience.
- [Endocrine inactive pituitary microadenomas: current data on natural history and follow-up approaches].
- Oxidative Phosphorylation in Silent Pituitary Adenomas: A Multiomics Perspective.
- Silent growth hormone pituitary adenomas: a single-center study.
- Characteristics and treatment of a silent somatotroph tumor that had transformed to a functional type: a case report and literature review.
- Suspected silent pituitary somatotroph neuroendocrine tumor associated with acromegaly-like bone disorders: a case report.
Bases de dados e fontes oficiais
Identificadores e referências canônicas usadas para montar este verbete.
- ORPHA:314786(Orphanet)
- MONDO:0017825(MONDO)
- GARD:21392(GARD (NIH))
- Variantes catalogadas(ClinVar)
- Busca completa no PubMed(PubMed)
- Q55787420(Wikidata)
Dados compilados pelo RarasNet a partir de fontes abertas (Orphanet, OMIM, MONDO, PubMed/EuropePMC, ClinicalTrials.gov, DATASUS, PCDT/MS). Este conteúdo é informativo e não substitui avaliação médica.
Conteúdo mantido por Agente Raras · Médicos e pesquisadores podem colaborar
Adenoma hipofisário silencioso
📋 Origem dos dados
Esta página agrega dados de fontes públicas e oficiais. Dados sobre cobertura no SUS (PCDT, CEAF) são verificados ativamente por agente proativo (ver badge no infobox). Demais dados têm atribuição de fonte + data da última sincronização — clique para abrir o original.
- Doença rara (ontologia)
- fonte: Orphanet
- Identificador unificado
- fonte: MONDO
- Codificação WHO/SUS
- fonte: WHO ICD-10 / DATASUS
- NIH/GARD
- fonte: GARD (NIH)
- Dado público estruturado
- fonte: Wikidata
- Ensaios clínicos
- fonte: ClinicalTrials.gov