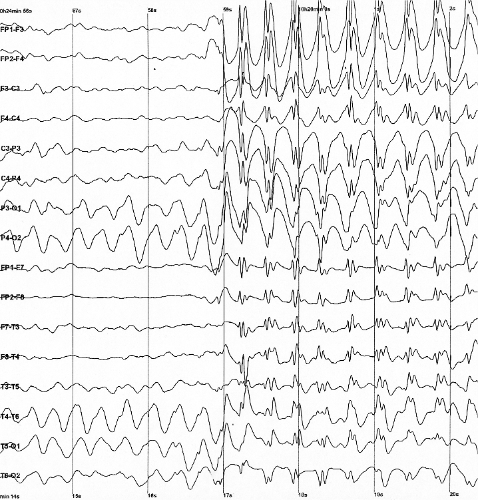
A epilepsia generalizada é uma forma de epilepsia caracterizada por crises generalizadas que ocorrem sem causa óbvia. As crises generalizadas, ao contrário das crises focais, são um tipo de convulsão que se manifesta com comprometimento da consciência, achados motores bilaterais ou ambos. As crises generalizadas também diferem das crises focais por se originarem em ambos os lados (hemisférios) do cérebro e distorcerem a atividade elétrica de todo o cérebro ou de uma porção maior dele. Esses achados elétricos são comumente visualizados no eletroencefalograma (EEG) como parte do diagnóstico.
Introdução
O que você precisa saber de cara
Visão geral
A Epilepsy with generalized tonic-clonic seizures alone é uma doença rara caracterizada exclusivamente por crises epilépticas generalizadas tônico-clônicas (antigamente chamadas de “grande mal”). Isso significa que as crises afetam ambos os hemisférios cerebrais desde o início, causando perda de consciência, rigidez muscular (fase tônica) e movimentos rítmicos (fase clônica). Não há outros tipos de crise associados. A condição é classificada no grupo das epilepsias generalizadas idiopáticas e tem código CID-10 G40.3.[1]
Sinais e sintomas
O principal e único sintoma são as crises tônico-clônicas generalizadas. Durante a crise, a pessoa perde a consciência subitamente, os músculos de todo o corpo enrijecem (fase tônica), seguidos por contrações rítmicas e simétricas dos braços e pernas (fase clônica). Pode ocorrer mordedura de língua, liberação esfincteriana e respiração ruidosa. Após a crise, há um período de confusão, sonolência e dor muscular (fase pós-ictal). Não há outros tipos de crise, como ausências ou crises focais.[1]
Causas genéticas
A base genética da Epilepsy with generalized tonic-clonic seizures alone ainda não foi completamente esclarecida. Até o momento, não há um gene específico ou padrão de herança claramente estabelecido para esta condição isoladamente. Estudos genéticos mais amplos (como sequenciamento do exoma) podem ser úteis para investigar possíveis variantes associadas, mas a causa genética permanece desconhecida na maioria dos casos.[1][3]
Diagnóstico
O diagnóstico é essencialmente clínico, baseado na descrição das crises tônico-clônicas generalizadas e na exclusão de outros tipos de crise. O eletroencefalograma (EEG) pode mostrar atividade epileptiforme generalizada, mas não é obrigatório para o diagnóstico. Exames de imagem (como ressonância magnética) são normais. No Brasil, o Sistema Único de Saúde (SUS) oferece cobertura parcial para o diagnóstico, incluindo o sequenciamento completo do exoma (WES) e atendimento em reabilitação para doenças raras, quando indicado.[1]
Tratamento e manejo
O tratamento é baseado no uso de medicamentos anticrises (antiepilépticos) para controlar as crises tônico-clônicas generalizadas. A escolha do medicamento deve ser individualizada, levando em conta a eficácia, efeitos colaterais e perfil do paciente. Entre os fármacos com potencial de uso estão: ácido aminohidroxibutírico, beclamida, carbamazepina, diclofenamida, eslicarbazepina, etosuximida, etotoína, felbamato, fosfenitoína, gabapentina, lamotrigina, levetiracetam, metarbital, fenacemida, piridoxal, stiripentol, topiramato, ácido valproico, valpromida e zonisamida. O tratamento deve ser acompanhado por neurologista. O SUS oferece cobertura parcial para medicamentos e procedimentos de reabilitação.[1]
Prognóstico e qualidade de vida
Com tratamento adequado, muitas pessoas conseguem controle satisfatório das crises, mantendo boa qualidade de vida. No entanto, crises não controladas podem impactar atividades diárias, como dirigir, trabalhar e estudar. O acompanhamento médico regular é fundamental para ajustar a medicação e monitorar possíveis efeitos adversos. O prognóstico a longo prazo é geralmente favorável, especialmente quando o diagnóstico é precoce e o tratamento é bem tolerado.[1]
Conteúdo informativo gerado e mantido automaticamente a partir de fontes oficiais (Orphanet, HPO, OMIM, SUS). Não substitui avaliação médica.
A epilepsia generalizada é uma forma de epilepsia caracterizada por crises generalizadas que ocorrem sem causa óbvia. As crises generalizadas, ao contrário das crises focais, são um tipo de convulsão que se manifesta com comprometimento da consciência, achados motores bilaterais ou ambos. As crises generalizadas também diferem das crises focais por se originarem em ambos os lados (hemisférios) do cérebro e distorcerem a atividade elétrica de todo o cérebro ou de uma porção maior dele. Esses achados elétricos são comumente visualizados no eletroencefalograma (EEG) como parte do diagnóstico.
Encontrou um erro ou informação desatualizada? Sugira uma correção →
Entender a doença
Do básico ao detalhe, leia no seu ritmo
Preparando trilha educativa...
Sinais e sintomas
O que aparece no corpo e com que frequência cada sintoma acontece
Visão geral
A Epilepsy with generalized tonic-clonic seizures alone é uma doença rara caracterizada exclusivamente por crises epilépticas generalizadas tônico-clônicas (antigamente chamadas de “grande mal”). Isso significa que as crises afetam ambos os hemisférios cerebrais desde o início, causando perda de consciência, rigidez muscular (fase tônica) e movimentos rítmicos (fase clônica). Não há outros tipos de crise associados. A condição é classificada no grupo das epilepsias generalizadas idiopáticas e tem código CID-10 G40.3.[1]
Sinais e sintomas
O principal e único sintoma são as crises tônico-clônicas generalizadas. Durante a crise, a pessoa perde a consciência subitamente, os músculos de todo o corpo enrijecem (fase tônica), seguidos por contrações rítmicas e simétricas dos braços e pernas (fase clônica). Pode ocorrer mordedura de língua, liberação esfincteriana e respiração ruidosa. Após a crise, há um período de confusão, sonolência e dor muscular (fase pós-ictal). Não há outros tipos de crise, como ausências ou crises focais.[1]
Causas genéticas
A base genética da Epilepsy with generalized tonic-clonic seizures alone ainda não foi completamente esclarecida. Até o momento, não há um gene específico ou padrão de herança claramente estabelecido para esta condição isoladamente. Estudos genéticos mais amplos (como sequenciamento do exoma) podem ser úteis para investigar possíveis variantes associadas, mas a causa genética permanece desconhecida na maioria dos casos.[1][3]
Diagnóstico
O diagnóstico é essencialmente clínico, baseado na descrição das crises tônico-clônicas generalizadas e na exclusão de outros tipos de crise. O eletroencefalograma (EEG) pode mostrar atividade epileptiforme generalizada, mas não é obrigatório para o diagnóstico. Exames de imagem (como ressonância magnética) são normais. No Brasil, o Sistema Único de Saúde (SUS) oferece cobertura parcial para o diagnóstico, incluindo o sequenciamento completo do exoma (WES) e atendimento em reabilitação para doenças raras, quando indicado.[1]
Tratamento e manejo
O tratamento é baseado no uso de medicamentos anticrises (antiepilépticos) para controlar as crises tônico-clônicas generalizadas. A escolha do medicamento deve ser individualizada, levando em conta a eficácia, efeitos colaterais e perfil do paciente. Entre os fármacos com potencial de uso estão: ácido aminohidroxibutírico, beclamida, carbamazepina, diclofenamida, eslicarbazepina, etosuximida, etotoína, felbamato, fosfenitoína, gabapentina, lamotrigina, levetiracetam, metarbital, fenacemida, piridoxal, stiripentol, topiramato, ácido valproico, valpromida e zonisamida. O tratamento deve ser acompanhado por neurologista. O SUS oferece cobertura parcial para medicamentos e procedimentos de reabilitação.[1]
Prognóstico e qualidade de vida
Com tratamento adequado, muitas pessoas conseguem controle satisfatório das crises, mantendo boa qualidade de vida. No entanto, crises não controladas podem impactar atividades diárias, como dirigir, trabalhar e estudar. O acompanhamento médico regular é fundamental para ajustar a medicação e monitorar possíveis efeitos adversos. O prognóstico a longo prazo é geralmente favorável, especialmente quando o diagnóstico é precoce e o tratamento é bem tolerado.[1]
Conteúdo informativo gerado e mantido automaticamente a partir de fontes oficiais (Orphanet, HPO, OMIM, SUS). Não substitui avaliação médica.
Linha do tempo da pesquisa
Encontrou um erro ou informação desatualizada? Sugira uma correção →
Genética e causas
O que está alterado no DNA e como passa nas famílias
Nenhum gene associado encontrado
Os dados genéticos desta condição ainda estão sendo catalogados.
Diagnóstico
Os sinais que médicos procuram e os exames que confirmam
Tratamento e manejo
Remédios, cuidados de apoio e o que precisa acompanhar
Onde tratar no SUS
Hospitais de referência no Brasil e o protocolo oficial do SUS (PCDT)
🇧🇷 Atendimento SUS — Epilepsy with generalized tonic-clonic seizures alone
Selecione um estado ou use sua localização para ver resultados.
Dados de DATASUS/CNES, SBGM, ABNeuro e Ministério da Saúde. Sempre confirme a disponibilidade diretamente com o estabelecimento.
Pesquisa ativa
Ensaios clínicos abertos e novidades científicas recentes
Ensaios em destaque
Pesquisa e ensaios clínicos
0 ensaios clínicos encontrados.
Publicações mais relevantes
Effect of Antiseizure Medication on the Salience Network in Patients with Epilepsy with Generalized Tonic-Clonic Seizures Alone.
This study aimed to investigate the effects of antiepileptic drugs on salience network regions in patients with epilepsy with generalized tonic-clonic seizures alone (EGTCSa). A retrospective observational case-control study was performed on 40 patients diagnosed with epilepsy with EGTCSa and 40 healthy age-matched controls. In LORETA, a voxel-by-voxel analysis between regions from the salience network was performed for both hemispheres, specifically between the anterior cingulate (BA 32 and BA 24) and the sublobar insula (BA 13). Subsequently, a Wilcoxon rank-sum test (the Mann-Whitney U test) was conducted for the equality of medians in the transformation matrix. A comparison was then made between each region of interest as defined by the salience network and the controls. Marked differences were found in the brain regions assessed in patients with EGTCSa treated with valproic acid and carbamazepine compared to the control group; few differences in patients treated with levetiracetam; and no difference was found in the group without treatment compared with those in the control group. These results suggest that ASMs can influence cognitive processes, which provide novel insights toward understanding the neural mechanisms underlying the effects of ASMs administration.
Oligoepilepsy and lifelong seizure susceptibility in epilepsy with generalized tonic-clonic seizures alone: Experience at an adult tertiary center.
Epilepsy with generalized tonic-clonic seizures alone (GTCA) is the least studied syndrome within the idiopathic generalized epilepsy (IGE) spectrum. We characterize a large cohort of adult patients with GTCA to understand natural history and drug responsiveness. In this retrospective single-center study using our epilepsy electronic record, we evaluated clinical characteristics, seizure outcomes, anti-seizure medication (ASM) response including seizure recurrence after ASM withdrawal, and sex differences in a cohort of GTCA patients aged ≥17 years. Within a cohort of 434 IGE patients, 87 patients (20 %) with GTCA were included. The mean age was 34.9 years (range 17-73 years). Forty-six patients (52.8 %) were females. Seventy-two patients (82.8 %) were seizure-free and 15 (17.2 %) had active epilepsy over the previous 12 months. Thirty-four patients (39.1 %) had ≤5 lifetime seizures, aligning with a prior definition of 'oligoepilepsy'. Sixty-five patients (74.7 %) were treated with monotherapy, 19 (21.8 %) were treated with polytherapy, and three were not taking any ASM. Levetiracetam (37.9 %) was the most commonly prescribed ASM, followed by lamotrigine (32.1 %) and valproate (31 %). Seventeen patients (19.5 %) attempted to withdraw their ASM. The rate of seizure recurrence after ASM withdrawal was 88.2 % (15/17), including two patients who relapsed more than 20 years after ASM discontinuation. Females had more seizures in their lifetime and had trialed more ASM compared to males. GTCA has a relatively good prognosis, with most patients becoming seizure-free on monotherapy. The high rate of seizure recurrence after ASM withdrawal supports lifetime seizure susceptibility. We found potential sex differences in seizure outcomes and ASM response, although further research is needed to validate this finding.
Recurrence rates and risk factors for seizure recurrence following antiseizure medication withdrawal in adolescent patients with genetic generalized epilepsy.
This study aimed to identify the recurrence rate of genetic generalized epilepsy (GGE) and risk factors for recurrence after antiseizure medication (ASM) withdrawal in adolescent patients. We retrospectively reviewed medical records of patients with GGE who were included in the registry at the Department of Child Neurology, National Hospital Organization Nishiniigata Chuo Hospital from 2000 through 2020. The eligibility criteria were as follows: onset of epileptic seizures at <15 years of age, treatment with an ASM, and attempted treatment withdrawal at 10-19 years of age. The rates of seizure recurrence after drug withdrawal were evaluated. Moreover, several variables were evaluated as predictors of recurrence. In total, 77 patients with GGE (21, 13, and 43 patients with juvenile myoclonic epilepsy [JME], juvenile absence epilepsy [JAE], and epilepsy with generalized tonic-clonic seizures alone [EGTCSA], respectively) were included in this study. Recurrence was detected in 68% of patients with GGE (86%, 31%, and 70% of patients with JME, JAE, and EGTCSA, respectively). Recurrence rates for patients who developed epilepsy at ≥13 years of age, those who started dose reduction at ≥16 years of age, those who exhibited a seizure-free period of <36 months before withdrawal, and those who chose to discontinue treatment at their own discretion were significantly higher than those for their counterparts. Multivariate analysis revealed that initiation of dose reduction at ≥16 years of age was associated with increased recurrence risk. Meanwhile, a diagnosis of JAE was associated with decreased recurrence risk. All patients with JAE were treated with valproic acid. Antiseizure medication withdrawal at ≥16 years of age and a diagnosis other than JAE may be independent risk factors for seizure recurrence after drug withdrawal in adolescent patients.
How to diagnose and classify idiopathic (genetic) generalized epilepsies.
Idiopathic or genetic generalized epilepsies (IGE) constitute an electroclinically well-defined group that accounts for almost one third of all people with epilepsy. They consist of four well-established syndromes and some other rarer phenotypes. The main four IGEs are juvenile myoclonic epilepsy, childhood absence epilepsy, juvenile absence epilepsy and IGE with generalized tonic-clonic seizures alone. There are three main seizure types in IGE, namely generalized tonic-clonic seizures, typical absences and myoclonic seizures, occurring either alone or in any combination. Diagnosing IGEs requires a multidimensional approach. The diagnostic process begins with a thorough medical history with a specific focus on seizure types, age at onset, timing and triggers. Comorbidities and family history should be questioned comprehensively. The EEG can provide valuable information for the diagnosis, including specific IGE syndromes, and therefore contribute to their optimal pharmacological treatment and management.
Long-term outcome in adolescent-onset generalized genetic epilepsies.
Until now, it has been unclear if the three subsyndromes of adolescent-onset generalized genetic epilepsy (GGE) differ in long-term prognosis. Therefore, this study aimed to compare long-term seizure outcome in juvenile absence epilepsy (JAE), juvenile myoclonic epilepsy (JME), and epilepsy with generalized tonic-clonic seizures alone (EGTCS). This retrospective study is based on the archive of an institutional tertiary care outpatient clinic for adult patients with epilepsy. Charts of 870 epilepsy outpatients were reviewed among whom 176 had adolescent-onset GGE (53 JAE, 66 JME, 57 EGTCS). Median patient age at investigation was 60 years; median follow-up time was 42.5 years. If possible, GGE patients were additionally interviewed on psychosocial and clinical variables. Age at first seizure was significantly higher in EGTCS patients (median 18 years) than in patients with JAE or JME (14 years each; p ≤ 0.001). Long-term seizure outcome hardly differed between the three subsyndromes. At the end of follow-up, 60% of all patients were in 5-year terminal seizure remission, and in 14%, epilepsy even had resolved (>10 years without seizures, >5 years without pharmacotherapy). Twenty percent of patients had persistent seizures during the last year of follow-up. Across all patients, 23% reported a psychiatric comorbidity, 87% had married, and 57% had achieved university entrance qualification. Long-term outcome was shown to be highly similar across all subsyndromes of adolescent-onset GGE. Even in a selection of difficult-to-treat epilepsy patients still attending an adult epilepsy clinic, most become seizure-free. To confirm these findings, prospective studies are needed.
Publicações recentes
Effect of Antiseizure Medication on the Salience Network in Patients with Epilepsy with Generalized Tonic-Clonic Seizures Alone.
Oligoepilepsy and lifelong seizure susceptibility in epilepsy with generalized tonic-clonic seizures alone: Experience at an adult tertiary center.
Recurrence rates and risk factors for seizure recurrence following antiseizure medication withdrawal in adolescent patients with genetic generalized epilepsy.
How to diagnose and classify idiopathic (genetic) generalized epilepsies.
Long-term outcome in adolescent-onset generalized genetic epilepsies.
📚 EuropePMC7 artigos no totalmostrando 5
Effect of Antiseizure Medication on the Salience Network in Patients with Epilepsy with Generalized Tonic-Clonic Seizures Alone.
BiomedicinesOligoepilepsy and lifelong seizure susceptibility in epilepsy with generalized tonic-clonic seizures alone: Experience at an adult tertiary center.
Epilepsy researchRecurrence rates and risk factors for seizure recurrence following antiseizure medication withdrawal in adolescent patients with genetic generalized epilepsy.
Epilepsia openHow to diagnose and classify idiopathic (genetic) generalized epilepsies.
Epileptic disorders : international epilepsy journal with videotapeLong-term outcome in adolescent-onset generalized genetic epilepsies.
EpilepsiaAssociações
Organizações que acompanham esta doença — pra ter apoio e orientação
Ainda não temos associações cadastradas para Epilepsy with generalized tonic-clonic seizures alone.
É de uma associação que acompanha esta doença? Fale com a gente →
Comunidades
Grupos ativos de quem convive com esta doença aqui no Raras
Ainda não existe comunidade no Raras para Epilepsy with generalized tonic-clonic seizures alone
Pacientes, familiares e cuidadores se organizam em comunidades pra compartilhar experiências, fazer perguntas e se apoiar. Você pode ser o primeiro.
Tire suas dúvidas
Perguntas, dicas e experiências compartilhadas aqui na página
Participe da discussão
Faça login para postar dúvidas, compartilhar experiências e interagir com especialistas.
Fazer loginDoenças relacionadas
Doenças com sintomas parecidos — ajudam quem ainda está buscando diagnóstico
Ainda não achamos doenças com sintomas parecidos o suficiente.
Referências e fontes
Bases de dados externas citadas neste artigo
Publicações científicas
Artigos indexados no PubMed ligados a esta doença no grafo RarasNet — título, periódico e PMID direto da fonte, sem intermediação de IA.
- Effect of Antiseizure Medication on the Salience Network in Patients with Epilepsy with Generalized Tonic-Clonic Seizures Alone.
- Oligoepilepsy and lifelong seizure susceptibility in epilepsy with generalized tonic-clonic seizures alone: Experience at an adult tertiary center.
- Recurrence rates and risk factors for seizure recurrence following antiseizure medication withdrawal in adolescent patients with genetic generalized epilepsy.
- How to diagnose and classify idiopathic (genetic) generalized epilepsies.
- Long-term outcome in adolescent-onset generalized genetic epilepsies.
Bases de dados e fontes oficiais
Identificadores e referências canônicas usadas para montar este verbete.
- ORPHA:698005(Orphanet)
- MONDO:0005754(MONDO)
- Epilepsia(PCDT · Ministério da Saúde)
- Busca completa no PubMed(PubMed)
Dados compilados pelo RarasNet a partir de fontes abertas (Orphanet, OMIM, MONDO, PubMed/EuropePMC, ClinicalTrials.gov, DATASUS, PCDT/MS). Este conteúdo é informativo e não substitui avaliação médica.
Conteúdo mantido por Agente Raras · Médicos e pesquisadores podem colaborar
Epilepsy with generalized tonic-clonic seizures alone
📋 Origem dos dados
Esta página agrega dados de fontes públicas e oficiais. Dados sobre cobertura no SUS (PCDT, CEAF) são verificados ativamente por agente proativo (ver badge no infobox). Demais dados têm atribuição de fonte + data da última sincronização — clique para abrir o original.
- Doença rara (ontologia)
- fonte: Orphanet
- Identificador unificado
- fonte: MONDO
- Codificação WHO/SUS
- fonte: WHO ICD-10 / DATASUS
- CID-11 (futuro)
- fonte: WHO ICD-11
- Indexação biomédica
- fonte: MeSH (NLM)
- Reposicionamento
- fonte: Drug Repurposing Hub