Doença autoimune progressiva que afeta o sistema nervoso central, resultando em desmielinização. Os pacientes desenvolvem deficiências físicas e cognitivas que correspondem às fibras nervosas afetadas.
Introdução
O que você precisa saber de cara
Doença autoimune progressiva que afeta o sistema nervoso central, resultando em desmielinização. Os pacientes desenvolvem deficiências físicas e cognitivas que correspondem às fibras nervosas afetadas.
Tem tratamento?
Encontrou um erro ou informação desatualizada? Sugira uma correção →
Entender a doença
Do básico ao detalhe, leia no seu ritmo
Preparando trilha educativa...
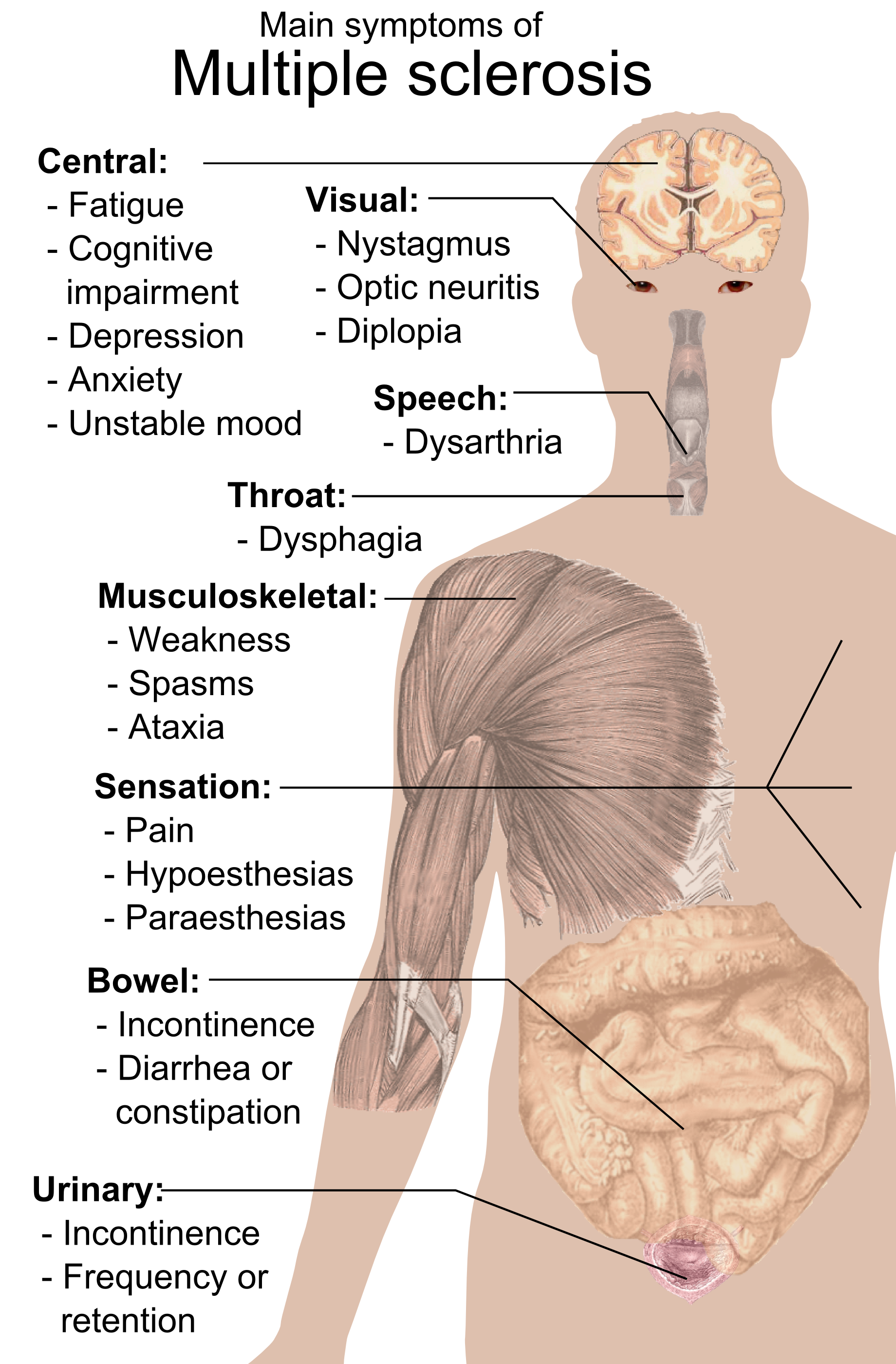
Sinais e sintomas
O que aparece no corpo e com que frequência cada sintoma acontece
Linha do tempo da pesquisa
Encontrou um erro ou informação desatualizada? Sugira uma correção →
Genética e causas
O que está alterado no DNA e como passa nas famílias
Genes associados
2 genes identificados com associação a esta condição.
Binds peptides derived from antigens that access the endocytic route of antigen presenting cells (APC) and presents them on the cell surface for recognition by the CD4 T-cells. The peptide binding cleft accommodates peptides of 10-30 residues. The peptides presented by MHC class II molecules are generated mostly by degradation of proteins that access the endocytic route, where they are processed by lysosomal proteases and other hydrolases. Exogenous antigens that have been endocytosed by the APC
Cell membraneEndoplasmic reticulum membraneGolgi apparatus, trans-Golgi network membraneEndosome membraneLysosome membrane
A beta chain of antigen-presenting major histocompatibility complex class II (MHCII) molecule. In complex with the alpha chain HLA-DRA, displays antigenic peptides on professional antigen presenting cells (APCs) for recognition by alpha-beta T cell receptor (TCR) on HLA-DRB1-restricted CD4-positive T cells. This guides antigen-specific T-helper effector functions, both antibody-mediated immune response and macrophage activation, to ultimately eliminate the infectious agents and transformed cells
Cell membraneEndoplasmic reticulum membraneLysosome membraneLate endosome membraneAutolysosome membrane
Medicamentos e terapias
Mecanismo: B-lymphocyte antigen CD20 binding agent
Mecanismo: Sphingosine 1-phosphate receptor Edg-1 agonist
Mecanismo: Interleukin-2 receptor inhibitor
Mecanismo: Integrin alpha-4/beta-7 inhibitor
Mecanismo: B-lymphocyte antigen CD20 binding agent
Mecanismo: Kelch-like ECH-associated protein 1 inhibitor
Mecanismo: B-lymphocyte antigen CD20 binding agent
Mecanismo: Kelch-like ECH-associated protein 1 inhibitor
Mecanismo: Dihydroorotate dehydrogenase inhibitor
Mecanismo: B-lymphocyte antigen CD19 binding agent
Variantes genéticas (ClinVar)
44 variantes patogênicas registradas no ClinVar.
Vias biológicas (Reactome)
7 vias biológicas associadas aos genes desta condição.
Diagnóstico
Os sinais que médicos procuram e os exames que confirmam
Tratamento e manejo
Remédios, cuidados de apoio e o que precisa acompanhar
Onde tratar no SUS
Hospitais de referência no Brasil e o protocolo oficial do SUS (PCDT)
🇧🇷 Atendimento SUS — NÃO RARA NA EUROPA: Esclerose múltipla
Selecione um estado ou use sua localização para ver resultados.
Dados de DATASUS/CNES, SBGM, ABNeuro e Ministério da Saúde. Sempre confirme a disponibilidade diretamente com o estabelecimento.
Pesquisa ativa
Ensaios clínicos abertos e novidades científicas recentes
Pesquisa e ensaios clínicos
Nenhum ensaio clínico registrado para esta condição.
Publicações mais relevantes
Adult-onset and late-onset multiple sclerosis in older adults in a Finnish university hospital.
The clinical characteristics of multiple sclerosis (MS) in individuals aged 65 years and older remain scarcely studied. This retrospective study compared late-onset MS (LOMS, onset ≥ 50 years) and adult-onset MS (AOMS, onset 18-49 years) in older adults with MS (OAwMS) aged ≥ 65 years. Data of subjects aged ≥ 65 years with a confirmed MS diagnosis and a recorded age at onset were collected from the Finnish MS registry at Tampere University Hospital, excluding individuals with paediatric-onset MS. Demographics, disease-modifying therapy (DMT) use, relapse history and Expanded Disability Status Scale (EDSS) scores were compared between LOMS and AOMS groups. The cohort included 248 subjects (41 LOMS, 207 AOMS). Primary progressive MS (PPMS) was more common in LOMS when compared to AOMS (41.5% vs. 12.6% at data acquisition, p < 0.001). Among subjects with a history of relapsing-remitting MS (RRMS) (32 LOMS, 178 AOMS), DMT had been used by 25.0% and 27.5% of subjects with LOMS and AOMS, and relapses after age 65 occurred in 18.8% and 7.3% of subjects with LOMS and AOMS, respectively. Subjects with LOMS discontinued DMT at an older age when compared to those with AOMS (mean 64.0 vs. 58.8 years, p = 0.04). No age-related differences in EDSS were observed after age 65. PPMS was more common among subjects with LOMS. Among subjects with a current or previous diagnosis of RRMS, occasional relapses were observed after age 65 in both groups, though multiple relapses were rare. These findings support the need for individualised care of OAwMS.
Evaluation of the methodology of independent Community Advisory Boards in health products research and development: a mixed-methods cross-sectional survey study.
Global burden of lower respiratory infections and aetiologies, 1990-2023: a systematic analysis for the Global Burden of Disease Study 2023.
Lower respiratory infections (LRIs) remain the world's leading infectious cause of death. This analysis from the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) 2023 provides global, regional, and national estimates of LRI incidence, mortality, and disability-adjusted life-years (DALYs), with attribution to 26 pathogens, including 11 newly modelled pathogens, across 204 countries and territories from 1990 to 2023. With new data and revised modelling techniques, these estimates serve as an update and expansion to GBD 2021. Through these estimates, we also aimed to assess progress towards the 2025 Global Action Plan for the Prevention and Control of Pneumonia and Diarrhoea (GAPPD) target for pneumonia mortality in children younger than 5 years. Mortality from LRIs, defined as physician-diagnosed pneumonia or bronchiolitis, was estimated using the Cause of Death Ensemble model with data from vital registration, verbal autopsy, surveillance, and minimally invasive tissue sampling. The Bayesian meta-regression tool DisMod-MR 2.1 was used to model overall morbidity due to LRIs. DALYs were calculated as the sum of years of life lost (YLLs) and years lived with disability (YLDs) for all locations, years, age groups, and sexes. We modelled pathogen-specific case-fatality ratios (CFRs) for each age group and location using splined binomial regression to create internally consistent estimates of incidence and mortality proportions attributable to viral, fungal, parasitic, and bacterial pathogens. Progress was assessed towards the GAPPD target of less than three deaths from pneumonia per 1000 livebirths, which is roughly equivalent to a mortality rate of less than 60 deaths per 100 000 children younger than 5 years. In 2023, LRIs were responsible for 2·50 million (95% uncertainty interval [UI] 2·24-2·81) deaths and 98·7 million (87·7-112) DALYs, with children younger than 5 years and adults aged 70 years and older carrying the highest burden. LRI mortality in children younger than 5 years fell by 33·4% (10·4-47·4) since 2010, with a global mortality rate of 94·8 (75·6-116·4) per 100 000 person-years in 2023. Among adults aged 70 years and older, the burden remained substantial with only marginal declines since 2010. A mortality rate of less than 60 deaths per 100 000 for children younger than 5 years was met by 129 of the 204 modelled countries in 2023. At a super-regional level, sub-Saharan Africa had an aggregate mortality rate in children younger than 5 years (hereafter referred to as under-5 mortality rate) furthest from the GAPPD target. Streptococcus pneumoniae continued to account for the largest number of LRI deaths globally (634 000 [95% UI 565 000-721 000] deaths or 25·3% [24·5-26·1] of all LRI deaths), followed by Staphylococcus aureus (271 000 [243 000-298 000] deaths or 10·9% [10·3-11·3]), and Klebsiella pneumoniae (228 000 [204 000-261 000] deaths or 9·1% [8·8-9·5]). Among pathogens newly modelled in this study, non-tuberculous mycobacteria (responsible for 177 000 [95% UI 155 000-201 000] deaths) and Aspergillus spp (responsible for 67 800 [59 900-75 900] deaths) emerged as important contributors. Altogether, the 11 newly modelled pathogens accounted for approximately 22% of LRI deaths. This comprehensive analysis underscores both the gains achieved through vaccination and the challenges that remain in controlling the LRI burden globally. Furthermore, it demonstrates persistent disparities in disease burden, with the highest mortality rates concentrated in countries in sub-Saharan Africa. Globally, as well as in these high-burden locations, the under-5 LRI mortality rate remains well above the GAPPD target. Progress towards this target requires equitable access to vaccines and preventive therapies-including newer interventions such as respiratory syncytial virus monoclonal antibodies-and health systems capable of early diagnosis and treatment. Expanding surveillance of emerging pathogens, strengthening adult immunisation programmes, and combating vaccine hesitancy are also crucial. As the global population ages, the dual challenge of sustaining gains in child survival while addressing the rising vulnerability in older adults will shape future pneumonia control strategies. Gates Foundation.
Global burden of 292 causes of death in 204 countries and territories and 660 subnational locations, 1990-2023: a systematic analysis for the Global Burden of Disease Study 2023.
Timely and comprehensive analyses of causes of death stratified by age, sex, and location are essential for shaping effective health policies aimed at reducing global mortality. The Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) 2023 provides cause-specific mortality estimates measured in counts, rates, and years of life lost (YLLs). GBD 2023 aimed to enhance our understanding of the relationship between age and cause of death by quantifying the probability of dying before age 70 years (70q0) and the mean age at death by cause and sex. This study enables comparisons of the impact of causes of death over time, offering a deeper understanding of how these causes affect global populations. GBD 2023 produced estimates for 292 causes of death disaggregated by age-sex-location-year in 204 countries and territories and 660 subnational locations for each year from 1990 until 2023. We used a modelling tool developed for GBD, the Cause of Death Ensemble model (CODEm), to estimate cause-specific death rates for most causes. We computed YLLs as the product of the number of deaths for each cause-age-sex-location-year and the standard life expectancy at each age. Probability of death was calculated as the chance of dying from a given cause in a specific age period, for a specific population. Mean age at death was calculated by first assigning the midpoint age of each age group for every death, followed by computing the mean of all midpoint ages across all deaths attributed to a given cause. We used GBD death estimates to calculate the observed mean age at death and to model the expected mean age across causes, sexes, years, and locations. The expected mean age reflects the expected mean age at death for individuals within a population, based on global mortality rates and the population's age structure. Comparatively, the observed mean age represents the actual mean age at death, influenced by all factors unique to a location-specific population, including its age structure. As part of the modelling process, uncertainty intervals (UIs) were generated using the 2·5th and 97·5th percentiles from a 250-draw distribution for each metric. Findings are reported as counts and age-standardised rates. Methodological improvements for cause-of-death estimates in GBD 2023 include a correction for the misclassification of deaths due to COVID-19, updates to the method used to estimate COVID-19, and updates to the CODEm modelling framework. This analysis used 55 761 data sources, including vital registration and verbal autopsy data as well as data from surveys, censuses, surveillance systems, and cancer registries, among others. For GBD 2023, there were 312 new country-years of vital registration cause-of-death data, 3 country-years of surveillance data, 51 country-years of verbal autopsy data, and 144 country-years of other data types that were added to those used in previous GBD rounds. The initial years of the COVID-19 pandemic caused shifts in long-standing rankings of the leading causes of global deaths: it ranked as the number one age-standardised cause of death at Level 3 of the GBD cause classification hierarchy in 2021. By 2023, COVID-19 dropped to the 20th place among the leading global causes, returning the rankings of the leading two causes to those typical across the time series (ie, ischaemic heart disease and stroke). While ischaemic heart disease and stroke persist as leading causes of death, there has been progress in reducing their age-standardised mortality rates globally. Four other leading causes have also shown large declines in global age-standardised mortality rates across the study period: diarrhoeal diseases, tuberculosis, stomach cancer, and measles. Other causes of death showed disparate patterns between sexes, notably for deaths from conflict and terrorism in some locations. A large reduction in age-standardised rates of YLLs occurred for neonatal disorders. Despite this, neonatal disorders remained the leading cause of global YLLs over the period studied, except in 2021, when COVID-19 was temporarily the leading cause. Compared to 1990, there has been a considerable reduction in total YLLs in many vaccine-preventable diseases, most notably diphtheria, pertussis, tetanus, and measles. In addition, this study quantified the mean age at death for all-cause mortality and cause-specific mortality and found noticeable variation by sex and location. The global all-cause mean age at death increased from 46·8 years (95% UI 46·6-47·0) in 1990 to 63·4 years (63·1-63·7) in 2023. For males, mean age increased from 45·4 years (45·1-45·7) to 61·2 years (60·7-61·6), and for females it increased from 48·5 years (48·1-48·8) to 65·9 years (65·5-66·3), from 1990 to 2023. The highest all-cause mean age at death in 2023 was found in the high-income super-region, where the mean age for females reached 80·9 years (80·9-81·0) and for males 74·8 years (74·8-74·9). By comparison, the lowest all-cause mean age at death occurred in sub-Saharan Africa, where it was 38·0 years (37·5-38·4) for females and 35·6 years (35·2-35·9) for males in 2023. Lastly, our study found that all-cause 70q0 decreased across each GBD super-region and region from 2000 to 2023, although with large variability between them. For females, we found that 70q0 notably increased from drug use disorders and conflict and terrorism. Leading causes that increased 70q0 for males also included drug use disorders, as well as diabetes. In sub-Saharan Africa, there was an increase in 70q0 for many non-communicable diseases (NCDs). Additionally, the mean age at death from NCDs was lower than the expected mean age at death for this super-region. By comparison, there was an increase in 70q0 for drug use disorders in the high-income super-region, which also had an observed mean age at death lower than the expected value. We examined global mortality patterns over the past three decades, highlighting-with enhanced estimation methods-the impacts of major events such as the COVID-19 pandemic, in addition to broader trends such as increasing NCDs in low-income regions that reflect ongoing shifts in the global epidemiological transition. This study also delves into premature mortality patterns, exploring the interplay between age and causes of death and deepening our understanding of where targeted resources could be applied to further reduce preventable sources of mortality. We provide essential insights into global and regional health disparities, identifying locations in need of targeted interventions to address both communicable and non-communicable diseases. There is an ever-present need for strengthened health-care systems that are resilient to future pandemics and the shifting burden of disease, particularly among ageing populations in regions with high mortality rates. Robust estimates of causes of death are increasingly essential to inform health priorities and guide efforts toward achieving global health equity. The need for global collaboration to reduce preventable mortality is more important than ever, as shifting burdens of disease are affecting all nations, albeit at different paces and scales. Gates Foundation.
Burden of 375 diseases and injuries, risk-attributable burden of 88 risk factors, and healthy life expectancy in 204 countries and territories, including 660 subnational locations, 1990-2023: a systematic analysis for the Global Burden of Disease Study 2023.
For more than three decades, the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) has provided a framework to quantify health loss due to diseases, injuries, and associated risk factors. This paper presents GBD 2023 findings on disease and injury burden and risk-attributable health loss, offering a global audit of the state of world health to inform public health priorities. This work captures the evolving landscape of health metrics across age groups, sexes, and locations, while reflecting on the remaining post-COVID-19 challenges to achieving our collective global health ambitions. The GBD 2023 combined analysis estimated years lived with disability (YLDs), years of life lost (YLLs), and disability-adjusted life-years (DALYs) for 375 diseases and injuries, and risk-attributable burden associated with 88 modifiable risk factors. Of the more than 310 000 total data sources used for all GBD 2023 (about 30% of which were new to this estimation round), more than 120 000 sources were used for estimation of disease and injury burden and 59 000 for risk factor estimation, and included vital registration systems, surveys, disease registries, and published scientific literature. Data were analysed using previously established modelling approaches, such as disease modelling meta-regression version 2.1 (DisMod-MR 2.1) and comparative risk assessment methods. Diseases and injuries were categorised into four levels on the basis of the established GBD cause hierarchy, as were risk factors using the GBD risk hierarchy. Estimates stratified by age, sex, location, and year from 1990 to 2023 were focused on disease-specific time trends over the 2010-23 period and presented as counts (to three significant figures) and age-standardised rates per 100 000 person-years (to one decimal place). For each measure, 95% uncertainty intervals [UIs] were calculated with the 2·5th and 97·5th percentile ordered values from a 250-draw distribution. Total numbers of global DALYs grew 6·1% (95% UI 4·0-8·1), from 2·64 billion (2·46-2·86) in 2010 to 2·80 billion (2·57-3·08) in 2023, but age-standardised DALY rates, which account for population growth and ageing, decreased by 12·6% (11·0-14·1), revealing large long-term health improvements. Non-communicable diseases (NCDs) contributed 1·45 billion (1·31-1·61) global DALYs in 2010, increasing to 1·80 billion (1·63-2·03) in 2023, alongside a concurrent 4·1% (1·9-6·3) reduction in age-standardised rates. Based on DALY counts, the leading level 3 NCDs in 2023 were ischaemic heart disease (193 million [176-209] DALYs), stroke (157 million [141-172]), and diabetes (90·2 million [75·2-107]), with the largest increases in age-standardised rates since 2010 occurring for anxiety disorders (62·8% [34·0-107·5]), depressive disorders (26·3% [11·6-42·9]), and diabetes (14·9% [7·5-25·6]). Remarkable health gains were made for communicable, maternal, neonatal, and nutritional (CMNN) diseases, with DALYs falling from 874 million (837-917) in 2010 to 681 million (642-736) in 2023, and a 25·8% (22·6-28·7) reduction in age-standardised DALY rates. During the COVID-19 pandemic, DALYs due to CMNN diseases rose but returned to pre-pandemic levels by 2023. From 2010 to 2023, decreases in age-standardised rates for CMNN diseases were led by rate decreases of 49·1% (32·7-61·0) for diarrhoeal diseases, 42·9% (38·0-48·0) for HIV/AIDS, and 42·2% (23·6-56·6) for tuberculosis. Neonatal disorders and lower respiratory infections remained the leading level 3 CMNN causes globally in 2023, although both showed notable rate decreases from 2010, declining by 16·5% (10·6-22·0) and 24·8% (7·4-36·7), respectively. Injury-related age-standardised DALY rates decreased by 15·6% (10·7-19·8) over the same period. Differences in burden due to NCDs, CMNN diseases, and injuries persisted across age, sex, time, and location. Based on our risk analysis, nearly 50% (1·27 billion [1·18-1·38]) of the roughly 2·80 billion total global DALYs in 2023 were attributable to the 88 risk factors analysed in GBD. Globally, the five level 3 risk factors contributing the highest proportion of risk-attributable DALYs were high systolic blood pressure (SBP), particulate matter pollution, high fasting plasma glucose (FPG), smoking, and low birthweight and short gestation-with high SBP accounting for 8·4% (6·9-10·0) of total DALYs. Of the three overarching level 1 GBD risk factor categories-behavioural, metabolic, and environmental and occupational-risk-attributable DALYs rose between 2010 and 2023 only for metabolic risks, increasing by 30·7% (24·8-37·3); however, age-standardised DALY rates attributable to metabolic risks decreased by 6·7% (2·0-11·0) over the same period. For all but three of the 25 leading level 3 risk factors, age-standardised rates dropped between 2010 and 2023-eg, declining by 54·4% (38·7-65·3) for unsafe sanitation, 50·5% (33·3-63·1) for unsafe water source, and 45·2% (25·6-72·0) for no access to handwashing facility, and by 44·9% (37·3-53·5) for child growth failure. The three leading level 3 risk factors for which age-standardised attributable DALY rates rose were high BMI (10·5% [0·1 to 20·9]), drug use (8·4% [2·6 to 15·3]), and high FPG (6·2% [-2·7 to 15·6]; non-significant). Our findings underscore the complex and dynamic nature of global health challenges. Since 2010, there have been large decreases in burden due to CMNN diseases and many environmental and behavioural risk factors, juxtaposed with sizeable increases in DALYs attributable to metabolic risk factors and NCDs in growing and ageing populations. This long-observed consequence of the global epidemiological transition was only temporarily interrupted by the COVID-19 pandemic. The substantially decreasing CMNN disease burden, despite the 2008 global financial crisis and pandemic-related disruptions, is one of the greatest collective public health successes known. However, these achievements are at risk of being reversed due to major cuts to development assistance for health globally, the effects of which will hit low-income countries with high burden the hardest. Without sustained investment in evidence-based interventions and policies, progress could stall or reverse, leading to widespread human costs and geopolitical instability. Moreover, the rising NCD burden necessitates intensified efforts to mitigate exposure to leading risk factors-eg, air pollution, smoking, and metabolic risks, such as high SBP, BMI, and FPG-including policies that promote food security, healthier diets, physical activity, and equitable and expanded access to potential treatments, such as GLP-1 receptor agonists. Decisive, coordinated action is needed to address long-standing yet growing health challenges, including depressive and anxiety disorders. Yet this can be only part of the solution. Our response to the NCD syndemic-the complex interaction of multiple health risks, social determinants, and systemic challenges-will define the future landscape of global health. To ensure human wellbeing, economic stability, and social equity, global action to sustain and advance health gains must prioritise reducing disparities by addressing socioeconomic and demographic determinants, ensuring equitable health-care access, tackling malnutrition, strengthening health systems, and improving vaccination coverage. We live in times of great opportunity. Gates Foundation and Bloomberg Philanthropies.
Publicações recentes
A cello concert in Brazilian lands: the life, art, and disease of Jacqueline du Pré.
Effect of 12 weeks of aquatic strength training on individuals with multiple sclerosis.
[Neuraxial anesthesia in patients with multiple sclerosis - a systematic review].
🥇 Revisão sistemáticaThe cerebrospinal fluid in multiple sclerosis: far beyond the bands.
📖 Revisão[Magnetic Resonance Imaging Conversion Predictors of Clinically Isolated Syndrome to Multiple Sclerosis].
📖 Revisão📚 EuropePMCmostrando 76
Evaluation of the methodology of independent Community Advisory Boards in health products research and development: a mixed-methods cross-sectional survey study.
Research involvement and engagementAdult-onset and late-onset multiple sclerosis in older adults in a Finnish university hospital.
Neurological sciences : official journal of the Italian Neurological Society and of the Italian Society of Clinical NeurophysiologyGlobal burden of lower respiratory infections and aetiologies, 1990-2023: a systematic analysis for the Global Burden of Disease Study 2023.
The Lancet. Infectious diseasesA narrative review on the safety of glatiramer acetate in multiple sclerosis: focus on Europe.
Therapeutic advances in chronic diseaseGlobal burden of 292 causes of death in 204 countries and territories and 660 subnational locations, 1990-2023: a systematic analysis for the Global Burden of Disease Study 2023.
Lancet (London, England)Burden of 375 diseases and injuries, risk-attributable burden of 88 risk factors, and healthy life expectancy in 204 countries and territories, including 660 subnational locations, 1990-2023: a systematic analysis for the Global Burden of Disease Study 2023.
Lancet (London, England)Smouldering disease in paediatric-onset multiple sclerosis.
EBioMedicineDeep Learning Modeling to Differentiate Multiple Sclerosis From MOG Antibody-Associated Disease.
NeurologyA narrative review of genetic and environmental factors and risk for multiple sclerosis. The design of the Italian multicentric PEDIGREE study.
Neurological sciences : official journal of the Italian Neurological Society and of the Italian Society of Clinical NeurophysiologyMultiple Sclerosis in the Greenlandic population. A nationwide cohort study.
Multiple sclerosis and related disordersGlobal, Regional, and National Burden of Nontraumatic Subarachnoid Hemorrhage: The Global Burden of Disease Study 2021.
JAMA neurologyVortioxetine in the routine management of major depressive disorder: an analysis of European automated healthcare databases.
Current medical research and opinionAzathioprine for people with multiple sclerosis.
The Cochrane database of systematic reviewsSafety of fingolimod in patients with relapsing remitting multiple sclerosis: A descriptive analysis of data from the EudraVigilance database.
Journal of the neurological sciencesAssociation of Autoimmune Diseases with the Risk of Parkinson's Disease.
NeuroepidemiologyAir pollution exposure and mortality from neurodegenerative diseases in the Netherlands: A population-based cohort study.
Environmental researchSafety and efficacy of arimoclomol in patients with early amyotrophic lateral sclerosis (ORARIALS-01): a randomised, double-blind, placebo-controlled, multicentre, phase 3 trial.
The Lancet. NeurologyComparison of Two Therapeutic Approaches of Cerebellar Transcranial Direct Current Stimulation in a Sardinian Family Affected by Spinocerebellar Ataxia 38: a Clinical and Computerized 3D Gait Analysis Study.
Cerebellum (London, England)A place for biosimilars in the changing multiple sclerosis treatment landscape.
Multiple sclerosis and related disordersInternational Delphi Consensus on the Management of AQP4-IgG+ NMOSD: Recommendations for Eculizumab, Inebilizumab, and Satralizumab.
Neurology(R) neuroimmunology & neuroinflammationMultiple sclerosis imaging in clinical practice: a European-wide survey of 428 centers and conclusions by the ESNR Working Group.
European radiologyA Whole-Genome Sequencing Study Implicates GRAMD1B in Multiple Sclerosis Susceptibility.
GenesA survey of genome-wide association studies, polygenic scores and UK Biobank highlights resources for autoimmune disease genetics.
Frontiers in immunologyRNA Helicases in Microsatellite Repeat Expansion Disorders and Neurodegeneration.
Frontiers in geneticsUse of Prescribed Drugs to Treat Chronic Diseases during Pregnancy in Outpatient Care in Switzerland between 2014 and 2018: Descriptive Analysis of Swiss Health Care Claims Data.
International journal of environmental research and public healthCerebrospinal fluid findings in COVID-19: a multicenter study of 150 lumbar punctures in 127 patients.
Journal of neuroinflammationBurden of rare coding variants in an Italian cohort of familial multiple sclerosis.
Journal of neuroimmunologyHomozygosity Haplotype and Whole-Exome Sequencing Analysis to Identify Potentially Functional Rare Variants Involved in Multiple Sclerosis among Sardinian Families.
Current issues in molecular biologySiponimod for multiple sclerosis.
The Cochrane database of systematic reviewsAn Investigation of the Role of Common and Rare Variants in a Large Italian Multiplex Family of Multiple Sclerosis Patients.
GenesObesity in Pediatric-Onset Multiple Sclerosis: A French Cohort Study.
Neurology(R) neuroimmunology & neuroinflammationDirect and indirect costs and cost-driving factors of Tuberous sclerosis complex in children, adolescents, and caregivers: a multicenter cohort study.
Orphanet journal of rare diseasesFamily-based exome sequencing identifies RBM45 as a possible candidate gene for frontotemporal dementia and amyotrophic lateral sclerosis.
Neurobiology of diseaseDirect and indirect costs and cost-driving factors in adults with tuberous sclerosis complex: a multicenter cohort study and a review of the literature.
Orphanet journal of rare diseasesRetention of antiseizure medications for epilepsy in multiple sclerosis: A retrospective observational study.
Epilepsy & behavior : E&BAn atlas of mitochondrial DNA genotype-phenotype associations in the UK Biobank.
Nature geneticsThe nature of genetic and environmental susceptibility to multiple sclerosis.
PloS oneUrban prevalence of multiple sclerosis in China: A population-based study in six provinces.
European journal of neurologyAnti-CD20 therapies and pregnancy in neuroimmunologic disorders: A cohort study from Germany.
Neurology(R) neuroimmunology & neuroinflammationChances and Challenges of Registry-Based Pharmacovigilance in Multiple Sclerosis: Lessons Learnt from the Implementation of the Multicenter REGIMS Registry.
Drug safetyNusinersen safety and effects on motor function in adult spinal muscular atrophy type 2 and 3.
Journal of neurology, neurosurgery, and psychiatryAn international discrete choice experiment assessing patients' preferences for disease-modifying therapy attributes in multiple sclerosis.
Neurodegenerative disease managementTreatment and outcome of aquaporin-4 antibody-positive NMOSD: A multinational pediatric study.
Neurology(R) neuroimmunology & neuroinflammationAntiphospholipid autoantibody detection is important in all patients with systemic autoimmune diseases.
Journal of autoimmunityThe retirement rate due to multiple sclerosis has decreased since 1995- A retrospective study in a Finnish central hospital.
Multiple sclerosis and related disordersNeurofibromatosis I and multiple sclerosis.
Orphanet journal of rare diseasesBurden of Rare Variants in ALS and Axonal Hereditary Neuropathy Genes Influence Survival in ALS: Insights from a Next Generation Sequencing Study of an Italian ALS Cohort.
International journal of molecular sciencesOligogenicity, C9orf72 expansion, and variant severity in ALS.
NeurogeneticsTargeted resequencing reveals rare variants enrichment in multiple sclerosis susceptibility genes.
Human mutationTowards a European health research and innovation cloud (HRIC).
Genome medicineThe Rare IL22RA2 Signal Peptide Coding Variant rs28385692 Decreases Secretion of IL-22BP Isoform-1, -2 and -3 and Is Associated with Risk for Multiple Sclerosis.
CellsPrimary progressive multiple sclerosis in a Russian cohort: relationship with gut bacterial diversity.
BMC microbiologyEvaluating the clinical effectiveness of autologous haematopoietic stem cell transplantation versus disease-modifying therapy in multiple sclerosis using a matching-adjusted indirect comparison: an exploratory study from the Autoimmune Diseases Working Party (ADWP) of the European Society of Bone and Marrow Transplantation (EBMT).
Bone marrow transplantationClinical and etiologic characteristics of de novo uveitis in patients aged 60 years and above: experience of a French tertiary center.
Graefe's archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle OphthalmologieThree VCP Mutations in Patients with Frontotemporal Dementia.
Journal of Alzheimer's disease : JADLinkage analysis and whole exome sequencing identify a novel candidate gene in a Dutch multiple sclerosis family.
Multiple sclerosis (Houndmills, Basingstoke, England)Genetic screening in early-onset dementia patients with unclear phenotype: relevance for clinical diagnosis.
Neurobiology of agingAssociation of a rare variant of the TNFSF13B gene with susceptibility to Rheumatoid Arthritis and Systemic Lupus Erythematosus.
Scientific reportsScreening for TSC1 and TSC2 mutations using NGS in Greek children with tuberous sclerosis syndrome.
European journal of paediatric neurology : EJPN : official journal of the European Paediatric Neurology SocietySeizures and Encephalitis in Myelin Oligodendrocyte Glycoprotein IgG Disease vs Aquaporin 4 IgG Disease.
JAMA neurologyPrevalence Estimates of Rare Congenital Anomalies by Integrating Two Population-Based Registries in Tuscany, Italy.
Public health genomicsPediatric-onset multiple sclerosis and other acquired demyelinating syndromes of the central nervous system in Denmark during 1977-2015: A nationwide population-based incidence study.
Multiple sclerosis (Houndmills, Basingstoke, England)Factors associated with adherence to disease modifying therapy in multiple sclerosis: An observational survey from a referral center in Lithuania.
Multiple sclerosis and related disordersThe effectiveness of Robot-Assisted Gait Training versus conventional therapy on mobility in severely disabled progressIve MultiplE sclerosis patients (RAGTIME): study protocol for a randomized controlled trial.
TrialsMortality and Causes of Death in Patients with Sporadic Inclusion Body Myositis: Survey Study Based on the Clinical Experience of Specialists in Australia, Europe and the USA.
Journal of neuromuscular diseasesTeriflunomide for multiple sclerosis.
The Cochrane database of systematic reviewsDevelopment and assessment of a website presenting evidence-based information for people with multiple sclerosis: the IN-DEEP project.
BMC neurologyATNX2 is not a regulatory gene in Italian amyotrophic lateral sclerosis patients with C9ORF72 GGGGCC expansion.
Neurobiology of agingNeuromyelitis optica spectrum disorders: comparison of clinical and magnetic resonance imaging characteristics of AQP4-IgG versus MOG-IgG seropositive cases in the Netherlands.
European journal of neurologyInvestigating the role of filamin C in Belgian patients with frontotemporal dementia linked to GRN deficiency in FTLD-TDP brains.
Acta neuropathologica communicationsMetabolomics as a diagnostic tool for idiopathic non-cirrhotic portal hypertension.
Liver international : official journal of the International Association for the Study of the LiverThe MS@Work study: a 3-year prospective observational study on factors involved with work participation in patients with relapsing-remitting Multiple Sclerosis.
BMC neurologyHFE p.H63D polymorphism does not influence ALS phenotype and survival.
Neurobiology of agingCumulative Review of Thrombotic Microangiopathy, Thrombotic Thrombocytopenic Purpura, and Hemolytic Uremic Syndrome Reports with Subcutaneous Interferon β-1a.
Advances in therapyDimethyl fumarate for multiple sclerosis.
The Cochrane database of systematic reviewsCHCH10 mutations in an Italian cohort of familial and sporadic amyotrophic lateral sclerosis patients.
Neurobiology of agingAssociações
Organizações que acompanham esta doença — pra ter apoio e orientação
Associação brasileira dedicada a Esclerose múltipla.
Comunidades
Grupos ativos de quem convive com esta doença aqui no Raras
Ainda não existe comunidade no Raras para NÃO RARA NA EUROPA: Esclerose múltipla
Pacientes, familiares e cuidadores se organizam em comunidades pra compartilhar experiências, fazer perguntas e se apoiar. Você pode ser o primeiro.
Tire suas dúvidas
Perguntas, dicas e experiências compartilhadas aqui na página
Participe da discussão
Faça login para postar dúvidas, compartilhar experiências e interagir com especialistas.
Fazer loginDoenças relacionadas
Doenças com sintomas parecidos — ajudam quem ainda está buscando diagnóstico
Ainda não achamos doenças com sintomas parecidos o suficiente.
Referências e fontes
Bases de dados externas citadas neste artigo
Publicações científicas
Artigos indexados no PubMed ligados a esta doença no grafo RarasNet — título, periódico e PMID direto da fonte, sem intermediação de IA.
- Adult-onset and late-onset multiple sclerosis in older adults in a Finnish university hospital.Neurological sciences : official journal of the Italian Neurological Society and of the Italian Society of Clinical Neurophysiology· 2026· PMID 41504984mais citado
- Evaluation of the methodology of independent Community Advisory Boards in health products research and development: a mixed-methods cross-sectional survey study.
- Global burden of lower respiratory infections and aetiologies, 1990-2023: a systematic analysis for the Global Burden of Disease Study 2023.
- Global burden of 292 causes of death in 204 countries and territories and 660 subnational locations, 1990-2023: a systematic analysis for the Global Burden of Disease Study 2023.
- Burden of 375 diseases and injuries, risk-attributable burden of 88 risk factors, and healthy life expectancy in 204 countries and territories, including 660 subnational locations, 1990-2023: a systematic analysis for the Global Burden of Disease Study 2023.
- A cello concert in Brazilian lands: the life, art, and disease of Jacqueline du Pré.
- Effect of 12 weeks of aquatic strength training on individuals with multiple sclerosis.
- [Neuraxial anesthesia in patients with multiple sclerosis - a systematic review].
- The cerebrospinal fluid in multiple sclerosis: far beyond the bands.
- [Magnetic Resonance Imaging Conversion Predictors of Clinically Isolated Syndrome to Multiple Sclerosis].
Bases de dados e fontes oficiais
Identificadores e referências canônicas usadas para montar este verbete.
- ORPHA:802(Orphanet)
- MONDO:0005301(MONDO)
- Esclerose Multipla(PCDT · Ministério da Saúde)
- Variantes catalogadas(ClinVar)
- Busca completa no PubMed(PubMed)
- Q55345657(Wikidata)
Dados compilados pelo RarasNet a partir de fontes abertas (Orphanet, OMIM, MONDO, PubMed/EuropePMC, ClinicalTrials.gov, DATASUS, PCDT/MS). Este conteúdo é informativo e não substitui avaliação médica.
Conteúdo mantido por Agente Raras · Médicos e pesquisadores podem colaborar