A deficiência de piruvato carboxilase (PC) infantil, do Tipo A, é uma forma rara e grave dessa condição. Ela se caracteriza por começar na infância, causar um acúmulo leve a moderado de ácido lático no sangue e, de modo geral, ter uma evolução grave.
Introdução
O que você precisa saber de cara
A deficiência de piruvato carboxilase (PC) infantil, do Tipo A, é uma forma rara e grave dessa condição. Ela se caracteriza por começar na infância, causar um acúmulo leve a moderado de ácido lático no sangue e, de modo geral, ter uma evolução grave.
Escala de raridade
<1/50kMuito rara
1/20kRara
1/10kPouco freq.
1/5kIncomum
1/2k
Encontrou um erro ou informação desatualizada? Sugira uma correção →
Entender a doença
Do básico ao detalhe, leia no seu ritmo
Preparando trilha educativa...
Sinais e sintomas
O que aparece no corpo e com que frequência cada sintoma acontece
Linha do tempo da pesquisa
Encontrou um erro ou informação desatualizada? Sugira uma correção →
Genética e causas
O que está alterado no DNA e como passa nas famílias
Genes associados
1 gene identificado com associação a esta condição. Padrão de herança: Autosomal recessive.
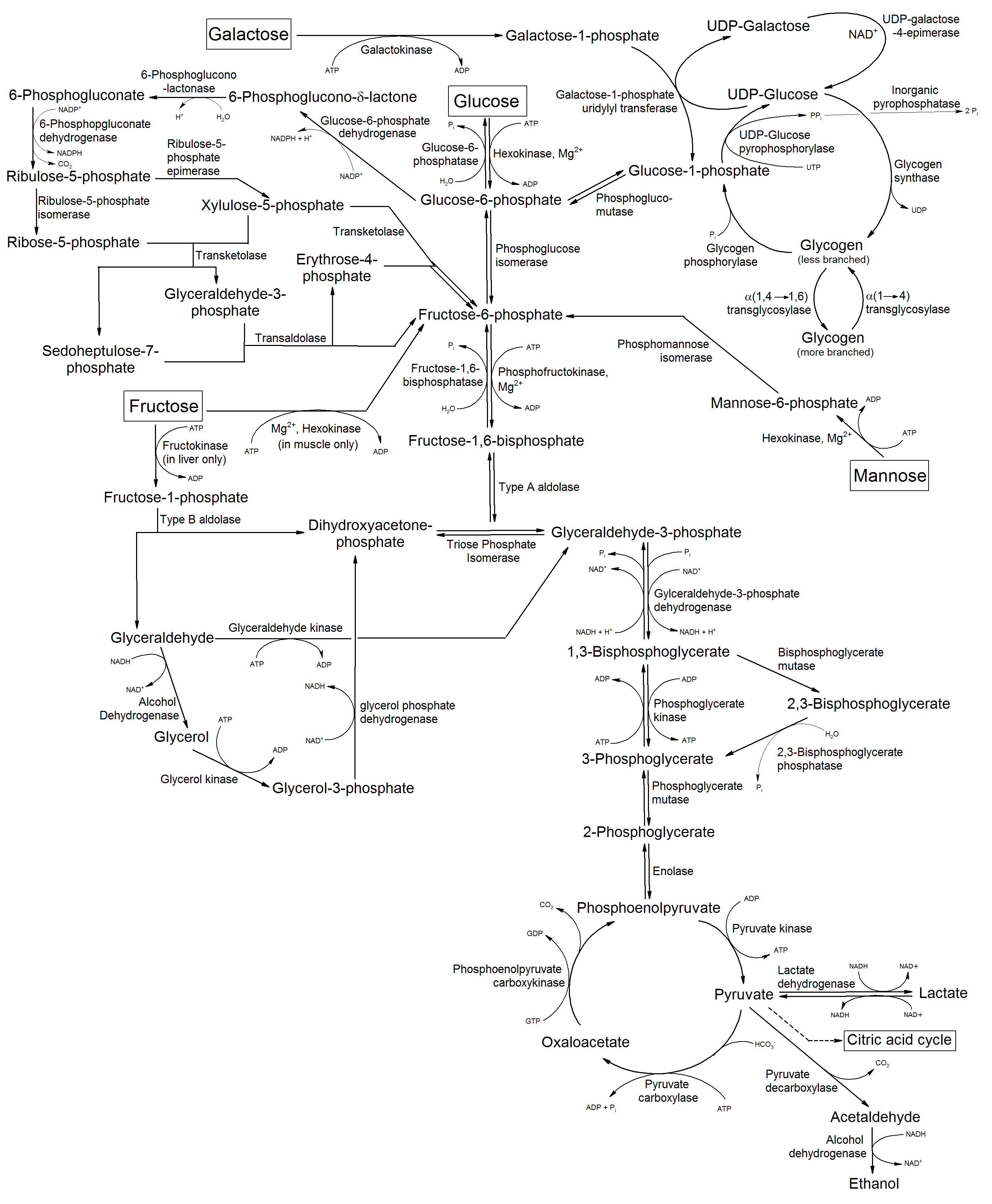
Pyruvate carboxylase catalyzes a 2-step reaction, involving the ATP-dependent carboxylation of the covalently attached biotin in the first step and the transfer of the carboxyl group to pyruvate in the second. Catalyzes in a tissue specific manner, the initial reactions of glucose (liver, kidney) and lipid (adipose tissue, liver, brain) synthesis from pyruvate
Mitochondrion matrix
Pyruvate carboxylase deficiency
Leads to lactic acidosis, intellectual disability and death. It occurs in three forms: mild or type A, severe neonatal or type B, and a very mild lacticacidemia.
Variantes genéticas (ClinVar)
286 variantes patogênicas registradas no ClinVar.
Vias biológicas (Reactome)
4 vias biológicas associadas aos genes desta condição.
Diagnóstico
Os sinais que médicos procuram e os exames que confirmam
Tratamento e manejo
Remédios, cuidados de apoio e o que precisa acompanhar
Onde tratar no SUS
Hospitais de referência no Brasil e o protocolo oficial do SUS (PCDT)
🇧🇷 Atendimento SUS — Deficiência de piruvato carboxilase, tipo infantil
Selecione um estado ou use sua localização para ver resultados.
Dados de DATASUS/CNES, SBGM, ABNeuro e Ministério da Saúde. Sempre confirme a disponibilidade diretamente com o estabelecimento.
Pesquisa ativa
Ensaios clínicos abertos e novidades científicas recentes
Pesquisa e ensaios clínicos
Nenhum ensaio clínico registrado para esta condição.
Publicações mais relevantes
Clinical, biochemical, and molecular profiles of three Sri Lankan neonates with pyruvate carboxylase deficiency.
Pyruvate carboxylase, a mitochondrial enzyme, catalyses the conversion of glycolytic end-product pyruvate to tricarboxylic acid cycle intermediate, oxaloacetate. Rare pyruvate carboxylase deficiency manifests in three clinical and biochemical phenotypes: neonatal onset type A, infantile onset type B and a benign C type. The objective of this case series is to expand the knowledge of overlapping clinical and biochemical phenotypes of pyruvate carboxylase deficiency. We report three Sri Lankan neonates including two siblings, of two unrelated families with pyruvate carboxylase deficiency. All three developed respiratory distress within the first few hours of birth. Two siblings displayed typical biochemical findings reported in type B. The other proband with normal citrulline, lysine, moderate lactate, paraventricular cystic lesions, bony deformities, and a novel missense, homozygous variant c.2746G>C [p.(Asp916His)] in the PC gene, biochemically favoured type A. Our findings indicate the necessity of prompt laboratory investigations in a tachypneic neonate with coexisting metabolic acidosis, as early recognition is essential for patient management and family counselling. Further case studies are required to identify overlapping symptoms and biochemical findings in different types of pyruvate carboxylase deficiency phenotypes. Pyruvate carboxylase (PC) deficiency is characterized in most affected individuals by failure to gain weight and/or linear growth failure, developmental delay, epilepsy, and metabolic acidosis. Three clinical phenotypes are recognized. Type A (infantile form) is characterized by infantile onset of metabolic and lactic acidosis, delayed motor development, intellectual disability, poor linear growth and/or weight gain, and neurologic findings (apathy, hypotonia, pyramidal and extrapyramidal signs, ataxia, and seizures). Brain anomalies can be noted. Most affected children die in infancy or early childhood. Type B (severe neonatal form) is characterized by neonatal or infantile onset of hypothermia, respiratory distress/failure, vomiting, severe lactic acidosis, hyperammonemia, and often hypoglycemia. Neurologic findings include brain abnormalities, lethargy, hypotonia, and pyramidal and extrapyramidal signs. Death typically occurs by age eight months. Type C (intermittent/attenuated form) is characterized by relatively normal or mildly delayed neurologic development, motor and/or gait abnormalities, (rarely) seizures, episodic movement disorders, and metabolic acidosis. Life span is unknown but survival into adulthood has been reported. The diagnosis of PC deficiency is established in a proband whose newborn screening or biochemical findings suggest PC deficiency based on identification of either (1) biallelic pathogenic variants in PC on molecular genetic testing or (2) PC deficiency in whole blood. Treatment of manifestations: Intravenous glucose-containing fluids, hydration, and correction of metabolic acidosis; pharmacologic therapies (amino acid supplements, cofactors, and vitamins) may improve some findings but not neurologic manifestations; orthotopic liver transplantation may be indicated in some affected individuals; anaplerotic therapies, such as triheptanoin, have had variable success (primarily for individuals with PC deficiency type C) but need further evaluation. Surveillance: A team of multidisciplinary specialists is often required to monitor existing manifestations, the individual's response to treatment, and the emergence of new manifestations. Agents/circumstances to avoid: A ketogenic diet is contraindicated, and it is critical to avoid fasting. Evaluation of relatives at risk: It is appropriate to clarify the genetic and/or biochemical status of apparently asymptomatic older and younger at-risk sibs of an affected individual with PC deficiency type C in order to identify as early as possible those who would benefit from prompt initiation of treatment and preventive measures. PC deficiency is inherited in an autosomal recessive manner. If both parents are known to be heterozygous for a PC pathogenic variant, each sib of an affected individual has at conception a 25% chance of inheriting biallelic pathogenic variants and being affected, a 50% chance of inheriting one pathogenic variant and being heterozygous, and a 25% chance of inheriting neither of the familial PC pathogenic variants. Once the PC pathogenic variants have been identified in an affected family member, molecular genetic carrier testing for at-risk relatives, prenatal testing, and preimplantation genetic testing are possible.
Prenatal onset of the neuroradiologic phenotype of pyruvate carboxylase deficiency due to homozygous PC c.1828G > A mutations.
Pyruvate carboxylase (PC) deficiency (MIM# 266150) is an autosomal recessive disorder with three subtypes. Patients homozygous for the c.1828G > A mutation in the PC gene belong to type A, which typically has infantile onset, severe to profound developmental delay, hypotonia, and lactic acidemia. We report the neuroimaging abnormalities in a 33-week gestation infant homozygous for the c.1828G > A mutation. Brain magnetic resonance imaging on day 10 of life revealed increased T2 signal within the subcortical and periventricular white matter, an immature gyral pattern, large periventricular cysts with mass effect on the lateral ventricles, and dilatation of the occipital and temporal horns. Magnetic resonance spectroscopy showed reduced creatine and NAA peaks, a relatively high choline peak and no lactate peak. These findings were observed prior to the neonate experiencing any episodes of decompensation with lactic acidosis. The presence of these brain anomalies at this gestational age, prior to any metabolic decompensation, supports the essential role of PC in normal brain morphogenesis and the resulting in-utero brain anomalies secondary to its deficiency. Our experience with this affected premature infant and many others we have managed with the same founder mutation suggests that the clinical phenotypes of the type A and the more severe type B PC deficient patients are on a spectrum rather than distinct subtypes.
Pyruvate carboxylase deficiency type A and type C: Characterization of five novel pathogenic variants in PC and analysis of the genotype-phenotype correlation.
Pyruvate carboxylase deficiency (PCD) is caused by biallelic mutations of the PC gene. The reported clinical spectrum includes a neonatal form with early death (type B), an infantile fatal form (type A), and a late-onset form with isolated mild intellectual delay (type C). Apart from homozygous stop-codon mutations leading to type B PCD, a genotype-phenotype correlation has not otherwise been discernible. Indeed, patients harboring biallelic heterozygous variants leading to PC activity near zero can present either with a fatal infantile type A or with a benign late onset type C form. In this study, we analyzed six novel patients with type A (three) and type C (three) PCD, and compared them with previously reported cases. First, we observed that type C PCD is not associated to homozygous variants in PC. In silico modeling was used to map former and novel variants associated to type A and C PCD, and to predict their potential effects on the enzyme structure and function. We found that variants lead to type A or type C phenotype based on the destabilization between the two major enzyme conformers. In general, our study on novel and previously reported patients improves the overall understanding on type A and C PCD.
Pyruvate Carboxylase Deficiency Type C: A Rare Cause of Acute Transient Flaccid Paralysis with Ketoacidosis.
Pyruvate carboxylase (PC) is a biotin-containing enzyme that is responsible for the adenosine triphosphate-dependent carboxylation of pyruvate to oxaloacetate, a key intermediate in the tricarboxylic acid cycle. PC deficiency (OMIM 266150) is a rare autosomal recessive metabolic disease, causing elevation of pyruvate, lactate, and alanine. Three types of PC deficiency have been described in the literature; A, B, and C. Type A PC deficiency, also called infantile or North American type, is characterized by infantile onset acidosis, failure to thrive, and developmental delay. The second subtype or type B, the neonatal or French form, presents usually in the neonatal period, mostly in the first 72 hours of life with severe lactic acidosis, truncal hypotonia, and seizures. The third type is called type C, is extremely rare with few cases published in the literature. In this case report, we present an 11-month-old girl who presented with acute flaccid paralysis, lethargy, and constipation with elevated ketones and lactate. She was confirmed genetically and biochemically to have PC deficiency type C. The patient's unusual presentation expands the clinical phenotype of this extremely rare disease.
Publicações recentes
Clinical, biochemical, and molecular profiles of three Sri Lankan neonates with pyruvate carboxylase deficiency.
Pyruvate Carboxylase Deficiency.
Pyruvate carboxylase deficiency type C; variable presentation and beneficial effect of triheptanoin.
In silico Analysis of Two Novel Variants in the Pyruvate Carboxylase (PC) Gene Associated with the Severe Form of PC Deficiency.
Case Report: Prenatal neurological injury in a neonate with pyruvate carboxylase deficiency type B.
📚 EuropePMCmostrando 4
Clinical, biochemical, and molecular profiles of three Sri Lankan neonates with pyruvate carboxylase deficiency.
Advances in laboratory medicinePrenatal onset of the neuroradiologic phenotype of pyruvate carboxylase deficiency due to homozygous PC c.1828G > A mutations.
JIMD reportsPyruvate carboxylase deficiency type A and type C: Characterization of five novel pathogenic variants in PC and analysis of the genotype-phenotype correlation.
Human mutationPyruvate Carboxylase Deficiency Type C: A Rare Cause of Acute Transient Flaccid Paralysis with Ketoacidosis.
NeuropediatricsAssociações
Organizações que acompanham esta doença — pra ter apoio e orientação
Ainda não temos associações cadastradas para Deficiência de piruvato carboxilase, tipo infantil.
É de uma associação que acompanha esta doença? Fale com a gente →
Comunidades
Grupos ativos de quem convive com esta doença aqui no Raras
Ainda não existe comunidade no Raras para Deficiência de piruvato carboxilase, tipo infantil
Pacientes, familiares e cuidadores se organizam em comunidades pra compartilhar experiências, fazer perguntas e se apoiar. Você pode ser o primeiro.
Tire suas dúvidas
Perguntas, dicas e experiências compartilhadas aqui na página
Participe da discussão
Faça login para postar dúvidas, compartilhar experiências e interagir com especialistas.
Fazer loginDoenças relacionadas
Doenças com sintomas parecidos — ajudam quem ainda está buscando diagnóstico
Ainda não achamos doenças com sintomas parecidos o suficiente.
Referências e fontes
Bases de dados externas citadas neste artigo
Publicações científicas
Artigos indexados no PubMed ligados a esta doença no grafo RarasNet — título, periódico e PMID direto da fonte, sem intermediação de IA.
- Clinical, biochemical, and molecular profiles of three Sri Lankan neonates with pyruvate carboxylase deficiency.
- Prenatal onset of the neuroradiologic phenotype of pyruvate carboxylase deficiency due to homozygous PC c.1828G > A mutations.
- Pyruvate carboxylase deficiency type A and type C: Characterization of five novel pathogenic variants in PC and analysis of the genotype-phenotype correlation.
- Pyruvate Carboxylase Deficiency Type C: A Rare Cause of Acute Transient Flaccid Paralysis with Ketoacidosis.
- Pyruvate Carboxylase Deficiency.
- Pyruvate carboxylase deficiency type C; variable presentation and beneficial effect of triheptanoin.
- In silico Analysis of Two Novel Variants in the Pyruvate Carboxylase (PC) Gene Associated with the Severe Form of PC Deficiency.
- Case Report: Prenatal neurological injury in a neonate with pyruvate carboxylase deficiency type B.
Bases de dados e fontes oficiais
Identificadores e referências canônicas usadas para montar este verbete.
- ORPHA:353308(Orphanet)
- MONDO:0018141(MONDO)
- GARD:17536(GARD (NIH))
- Variantes catalogadas(ClinVar)
- Busca completa no PubMed(PubMed)
- Q56014097(Wikidata)
Dados compilados pelo RarasNet a partir de fontes abertas (Orphanet, OMIM, MONDO, PubMed/EuropePMC, ClinicalTrials.gov, DATASUS, PCDT/MS). Este conteúdo é informativo e não substitui avaliação médica.
Conteúdo mantido por Agente Raras · Médicos e pesquisadores podem colaborar
Deficiência de piruvato carboxilase, tipo infantil
📋 Origem dos dados
Esta página agrega dados de fontes públicas e oficiais. Dados sobre cobertura no SUS (PCDT, CEAF) são verificados ativamente por agente proativo (ver badge no infobox). Demais dados têm atribuição de fonte + data da última sincronização — clique para abrir o original.
- Doença rara (ontologia)
- fonte: Orphanet
- Identificador unificado
- fonte: MONDO
- Codificação WHO/SUS
- fonte: WHO ICD-10 / DATASUS
- CID-11 (futuro)
- fonte: WHO ICD-11
- NIH/GARD
- fonte: GARD (NIH)
- Dado público estruturado
- fonte: Wikidata