Paralisia congênita do nervo oculomotor é uma condição rara presente ao nascimento, caracterizada pela fraqueza ou ausência de movimento em um ou ambos os olhos devido a um defeito no terceiro nervo craniano. Isso pode resultar em ptose (pálpebra caída) e estrabismo, afetando a visão binocular e a capacidade de seguir objetos.
Introdução
O que você precisa saber de cara
Visão geral
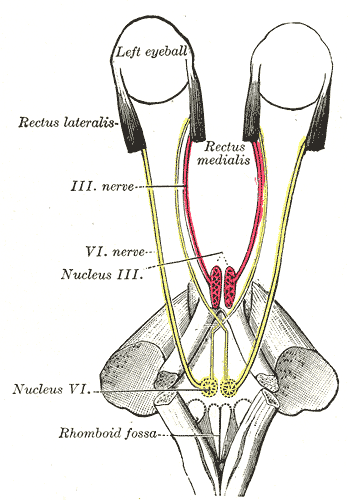
A paralisia congênita do nervo oculomotor é uma condição rara presente desde o nascimento (neonatal), caracterizada pela paralisia ou fraqueza dos músculos controlados pelo terceiro par craniano (nervo oculomotor). Isso afeta a movimentação do olho, a abertura da pálpebra e a resposta da pupila à luz. A condição é geralmente isolada, mas pode estar associada a outras alterações neurológicas ou síndromes genéticas.[1]
Sinais e sintomas
Os sinais aparecem logo após o nascimento e incluem: ptose (pálpebra caída), desvio do olho para fora e para baixo (exotropia e hipotropia), limitação dos movimentos oculares para cima, para baixo e para dentro, e, em alguns casos, dilatação da pupila com resposta lenta ou ausente à luz. A visão binocular pode ser comprometida, aumentando o risco de ambliopia (olho preguiçoso).[1]
Causas genéticas
A causa genética da paralisia congênita do nervo oculomotor ainda não foi completamente elucidada. Até o momento, nenhum gene específico foi confirmado como responsável pela condição. Acredita-se que possa estar relacionada a mutações em genes envolvidos no desenvolvimento do tronco cerebral ou dos nervos cranianos, mas as evidências são limitadas.[1][3]
Diagnóstico
O diagnóstico é clínico, baseado na observação dos sinais oculares ao nascimento. Exames complementares podem ser solicitados para descartar outras causas ou síndromes associadas. No Brasil, o Sistema Único de Saúde (SUS) oferece cobertura parcial para procedimentos como cariótipo (bandas G, Q ou R), pesquisa de microdeleções/microduplicações por FISH, sequenciamento completo do exoma (WES) e dosagem de alfa-fetoproteína. O atendimento em reabilitação para doenças raras também está disponível.[1]
Tratamento e manejo
O manejo é multidisciplinar e visa corrigir ou compensar os déficits oculares. Pode incluir uso de óculos com prismas, oclusão do olho saudável para prevenir ambliopia, e cirurgia de estrabismo ou ptose quando indicado. O acompanhamento com oftalmologista, neurologista e equipe de reabilitação é essencial. Não há medicamentos específicos aprovados para a condição.[1]
Prognóstico e qualidade de vida
O prognóstico depende da gravidade da paralisia e da presença de outras condições associadas. Com intervenção precoce e reabilitação adequada, muitas crianças conseguem desenvolver boa visão e qualidade de vida. No entanto, a paralisia pode ser permanente e exigir adaptações ao longo da vida.[1]
Conteúdo informativo gerado e mantido automaticamente a partir de fontes oficiais (Orphanet, HPO, OMIM, SUS). Não substitui avaliação médica.
Paralisia congênita do nervo oculomotor é uma condição rara presente ao nascimento, caracterizada pela fraqueza ou ausência de movimento em um ou ambos os olhos devido a um defeito no terceiro nervo craniano. Isso pode resultar em ptose (pálpebra caída) e estrabismo, afetando a visão binocular e a capacidade de seguir objetos.
Encontrou um erro ou informação desatualizada? Sugira uma correção →
Entender a doença
Do básico ao detalhe, leia no seu ritmo
Preparando trilha educativa...
Sinais e sintomas
O que aparece no corpo e com que frequência cada sintoma acontece
Visão geral
A paralisia congênita do nervo oculomotor é uma condição rara presente desde o nascimento (neonatal), caracterizada pela paralisia ou fraqueza dos músculos controlados pelo terceiro par craniano (nervo oculomotor). Isso afeta a movimentação do olho, a abertura da pálpebra e a resposta da pupila à luz. A condição é geralmente isolada, mas pode estar associada a outras alterações neurológicas ou síndromes genéticas.[1]
Sinais e sintomas
Os sinais aparecem logo após o nascimento e incluem: ptose (pálpebra caída), desvio do olho para fora e para baixo (exotropia e hipotropia), limitação dos movimentos oculares para cima, para baixo e para dentro, e, em alguns casos, dilatação da pupila com resposta lenta ou ausente à luz. A visão binocular pode ser comprometida, aumentando o risco de ambliopia (olho preguiçoso).[1]
Causas genéticas
A causa genética da paralisia congênita do nervo oculomotor ainda não foi completamente elucidada. Até o momento, nenhum gene específico foi confirmado como responsável pela condição. Acredita-se que possa estar relacionada a mutações em genes envolvidos no desenvolvimento do tronco cerebral ou dos nervos cranianos, mas as evidências são limitadas.[1][3]
Diagnóstico
O diagnóstico é clínico, baseado na observação dos sinais oculares ao nascimento. Exames complementares podem ser solicitados para descartar outras causas ou síndromes associadas. No Brasil, o Sistema Único de Saúde (SUS) oferece cobertura parcial para procedimentos como cariótipo (bandas G, Q ou R), pesquisa de microdeleções/microduplicações por FISH, sequenciamento completo do exoma (WES) e dosagem de alfa-fetoproteína. O atendimento em reabilitação para doenças raras também está disponível.[1]
Tratamento e manejo
O manejo é multidisciplinar e visa corrigir ou compensar os déficits oculares. Pode incluir uso de óculos com prismas, oclusão do olho saudável para prevenir ambliopia, e cirurgia de estrabismo ou ptose quando indicado. O acompanhamento com oftalmologista, neurologista e equipe de reabilitação é essencial. Não há medicamentos específicos aprovados para a condição.[1]
Prognóstico e qualidade de vida
O prognóstico depende da gravidade da paralisia e da presença de outras condições associadas. Com intervenção precoce e reabilitação adequada, muitas crianças conseguem desenvolver boa visão e qualidade de vida. No entanto, a paralisia pode ser permanente e exigir adaptações ao longo da vida.[1]
Conteúdo informativo gerado e mantido automaticamente a partir de fontes oficiais (Orphanet, HPO, OMIM, SUS). Não substitui avaliação médica.
Linha do tempo da pesquisa
Encontrou um erro ou informação desatualizada? Sugira uma correção →
Genética e causas
O que está alterado no DNA e como passa nas famílias
Nenhum gene associado encontrado
Os dados genéticos desta condição ainda estão sendo catalogados.
Diagnóstico
Os sinais que médicos procuram e os exames que confirmam
Tratamento e manejo
Remédios, cuidados de apoio e o que precisa acompanhar
Onde tratar no SUS
Hospitais de referência no Brasil e o protocolo oficial do SUS (PCDT)
🇧🇷 Atendimento SUS — Paralisia congênita do nervo oculomotor
Centros de Referência SUS
24 centros habilitados pelo SUS para Paralisia congênita do nervo oculomotor
Centros para Paralisia congênita do nervo oculomotor
Detalhes dos centros
Hospital Universitário Prof. Edgard Santos (HUPES)
R. Dr. Augusto Viana, s/n - Canela, Salvador - BA, 40110-060 · CNES 0003808
Serviço de Referência
Hospital Infantil Albert Sabin
R. Tertuliano Sales, 544 - Vila União, Fortaleza - CE, 60410-794 · CNES 2407876
Serviço de Referência
Hospital de Apoio de Brasília (HAB)
AENW 3 Lote A Setor Noroeste - Plano Piloto, Brasília - DF, 70684-831 · CNES 0010456
Serviço de Referência
Hospital Estadual Infantil e Maternidade Alzir Bernardino Alves (HIABA)
Av. Min. Salgado Filho, 918 - Soteco, Vila Velha - ES, 29106-010 · CNES 6631207
Serviço de Referência
Hospital das Clínicas da UFG
Rua 235 QD. 68 Lote Área, Nº 285, s/nº - Setor Leste Universitário, Goiânia - GO, 74605-050 · CNES 2338424
Serviço de Referência
Hospital Universitário da UFJF
R. Catulo Breviglieri, Bairro - s/n - Santa Catarina, Juiz de Fora - MG, 36036-110 · CNES 2297442
Atenção Especializada
Hospital das Clínicas da UFMG
Av. Prof. Alfredo Balena, 110 - Santa Efigênia, Belo Horizonte - MG, 30130-100 · CNES 2280167
Serviço de Referência
Hospital Universitário Julio Müller (HUJM)
R. Luis Philippe Pereira Leite, s/n - Alvorada, Cuiabá - MT, 78048-902 · CNES 2726092
Atenção Especializada
Hospital Universitário João de Barros Barreto
R. dos Mundurucus, 4487 - Guamá, Belém - PA, 66073-000 · CNES 2337878
Serviço de Referência
Hospital Universitário Lauro Wanderley (HULW)
R. Tabeliao Estanislau Eloy, 585 - Castelo Branco, João Pessoa - PB, 58050-585 · CNES 0002470
Atenção Especializada
Instituto de Medicina Integral Prof. Fernando Figueira (IMIP)
R. dos Coelhos, 300 - Boa Vista, Recife - PE, 50070-902 · CNES 0000647
Serviço de Referência
Hospital Pequeno Príncipe
R. Des. Motta, 1070 - Água Verde, Curitiba - PR, 80250-060 · CNES 3143805
Serviço de Referência
Hospital Universitário Regional de Maringá (HUM)
Av. Mandacaru, 1590 - Parque das Laranjeiras, Maringá - PR, 87083-240 · CNES 2216108
Atenção Especializada
Hospital de Clínicas da UFPR
R. Gen. Carneiro, 181 - Alto da Glória, Curitiba - PR, 80060-900 · CNES 2364980
Serviço de Referência
Hospital Universitário Pedro Ernesto (HUPE-UERJ)
Blvd. 28 de Setembro, 77 - Vila Isabel, Rio de Janeiro - RJ, 20551-030 · CNES 2280221
Serviço de Referência
Instituto Nacional de Saúde da Mulher, da Criança e do Adolescente Fernandes Figueira (IFF/Fiocruz)
Av. Rui Barbosa, 716 - Flamengo, Rio de Janeiro - RJ, 22250-020 · CNES 2269988
Serviço de Referência
Hospital São Lucas da PUCRS
Av. Ipiranga, 6690 - Jardim Botânico, Porto Alegre - RS, 90610-000 · CNES 2232928
Serviço de Referência
Hospital de Clínicas de Porto Alegre (HCPA)
Rua Ramiro Barcelos, 2350 Bloco A - Av. Protásio Alves, 211 - Bloco B e C - Santa Cecília, Porto Alegre - RS, 90035-903 · CNES 2237601
Serviço de Referência
Hospital Universitário da UFSC (HU-UFSC)
R. Profa. Maria Flora Pausewang - Trindade, Florianópolis - SC, 88036-800 · CNES 2560356
Serviço de Referência
Hospital das Clínicas da FMUSP
R. Dr. Ovídio Pires de Campos, 225 - Cerqueira César, São Paulo - SP, 05403-010 · CNES 2077485
Serviço de Referência
Hospital de Base de São José do Rio Preto
Av. Brg. Faria Lima, 5544 - Vila Sao Jose, São José do Rio Preto - SP, 15090-000 · CNES 2079798
Atenção Especializada
Hospital de Clínicas da UNICAMP
R. Vital Brasil, 251 - Cidade Universitária, Campinas - SP, 13083-888 · CNES 2748223
Serviço de Referência
Hospital de Clínicas de Ribeirão Preto (HCRP-USP)
R. Ten. Catão Roxo, 3900 - Vila Monte Alegre, Ribeirão Preto - SP, 14015-010 · CNES 2082187
Serviço de Referência
UNIFESP / Hospital São Paulo
R. Napoleão de Barros, 715 - Vila Clementino, São Paulo - SP, 04024-002 · CNES 2688689
Serviço de Referência
Dados de DATASUS/CNES, SBGM, ABNeuro e Ministério da Saúde. Sempre confirme a disponibilidade diretamente com o estabelecimento.
Pesquisa ativa
Ensaios clínicos abertos e novidades científicas recentes
Ensaios em destaque
🟢 Recrutando agora
2 pesquisas recrutando participantes. Converse com seu médico sobre a possibilidade de participar.
Outros ensaios clínicos
0 ensaios clínicos encontrados.
Publicações mais relevantes
Congenital oculomotor nerve palsy with aberrant eyelid movements and pupillary spasms: a case report.
We report a case of congenital oculomotor nerve palsy presenting with aberrant eyelid movements and an involuntary pupillary reaction. A 24-year-old woman presented with mild anisocoria with no significant medical history. Her ocular history included a history of strabismus and levator muscle surgery. Examination revealed exotropia, hypotropia, and ocular motility impairment, consistent with right oculomotor nerve palsy. Pupillary examination revealed mild anisocoria with the right pupil being unreactive to dim light, followed by involuntary pupillary spasms unassociated with eye position. Twitch-like movements of the upper eyelid were also observed during the spasm phase. Orbital magnetic resonance imaging revealed atrophy of the extraocular muscles, particularly the medial rectus. No intracranial lesions were found and blood tests excluded conditions such as thyroid eye disease. Based on these findings, congenital oculomotor nerve palsy with aberrant regeneration was diagnosed. The patient remained asymptomatic and was managed conservatively. Six months later, no complications due to pupillary spasms or restriction of ocular motility were observed. This case highlights an unusual pupillary response in congenital oculomotor nerve palsy characterized by involuntary pupillary spasms accompanied by upper eyelid twitching, which has not been previously reported. The prognosis was likely favorable for asymptomatic patients without associated underlying causes.
Magnetic Resonance Imaging in 14 Patients with Congenital Oculomotor Nerve Palsy.
To elucidate the imaging findings of congenital oculomotor nerve palsy by evaluating the oculomotor nerve and extraocular muscles on magnetic resonance (MR) imaging in a relatively large series of 14 patients with congenital oculomotor nerve palsy. Ophthalmologic examination of 14 consecutive patients diagnosed with congenital oculomotor nerve palsy, and MR imaging of the orbit and oculomotor nerves were performed. Of the 14 patients with congenital oculomotor nerve palsy, 13 patients (93%) were unilateral and 12 patients (86%) had incomplete palsy. On MR imaging, 5 patients (36%) had hypoplasia or aplasia of the oculomotor nerve with variable degrees of extraocular muscle atrophy on the affected side. Of the 14 patients, nine (64%) had normal-sized oculomotor nerves with or without muscle atrophy. The most frequently involved muscles were the inferior rectus (64%) and medial rectus (50%), followed by the superior rectus (29%) and inferior oblique muscles (14%). None of the 14 patients showed an abnormal abducens nerve. Congenital oculomotor nerve palsy was mostly incomplete and hypoplasia or aplasia of the oculomotor nerve was apparent in one third of patients showing variable degrees of extraocular muscle atrophy, mostly of the medial rectus and inferior rectus muscles.
A modified technique for attaching the lateral rectus muscle to the orbital periosteum through a skin incision over the lateral orbital rim.
The traditional approach for periosteal fixation of the lateral rectus muscle involves securing the muscle using nonabsorbable sutures by exposing the orbital periosteum 5 mm to the inside of the orbital margin. We present a simplified approach that exposes the orbital periosteum through a skin incision, providing more room and avoiding extraconal fat manipulation. We used our technique to expose the lateral orbital periosteum and suture the lateral rectus muscle to the periosteum using nonabsorbable sutures in 2 patients with exotropic Duane retraction syndrome and 1 patient with congenital oculomotor nerve palsy. All 3 patients had satisfactory postoperative alignment, with abduction limitation of 3-. Adduction improved in all patients. The patient with oculomotor nerve palsy had a small overcorrection in primary position that remained stable during follow-up of 18 months. There were no intraoperative complications. This modified approach to extraocular muscle periosteal fixation may be simpler than the standard approach. Further evaluation in a larger series of patients is warranted.
Imaging of Cranial Nerves III, IV, VI in Congenital Cranial Dysinnervation Disorders.
Congenital cranial dysinnervation disorders are a group of diseases caused by abnormal development of cranial nerve nuclei or their axonal connections, resulting in aberrant innervation of the ocular and facial musculature. Its diagnosis could be facilitated by the development of high resolution thin-section magnetic resonance imaging. The purpose of this review is to describe the method to visualize cranial nerves III, IV, and VI and to present the imaging findings of congenital cranial dysinnervation disorders including congenital oculomotor nerve palsy, congenital trochlear nerve palsy, Duane retraction syndrome, Möbius syndrome, congenital fibrosis of the extraocular muscles, synergistic divergence, and synergistic convergence.
Multiple Pathological Ocular Findings in a Patient With PHACE Syndrome.
The authors describe a 2-year-old girl diagnosed as having posterior fossa malformations, hemangiomas, arterial anomalies, cardiac anomalies, and eye abnormalities (PHACE) syndrome that presented with a large facial hemangioma of the forehead and eyelid, ptosis, microphthalmia, persistent pupillary membrane and pupillary ectopia, congenital oculomotor nerve palsy of the affected eye, and bilateral optic disc dysplasia. [J Pediatr Ophthalmol Strabismus. 2016;53:e72-e74.].
Publicações recentes
Congenital oculomotor nerve palsy with aberrant eyelid movements and pupillary spasms: a case report.
A modified technique for attaching the lateral rectus muscle to the orbital periosteum through a skin incision over the lateral orbital rim.
Magnetic Resonance Imaging in 14 Patients with Congenital Oculomotor Nerve Palsy.
Imaging of Cranial Nerves III, IV, VI in Congenital Cranial Dysinnervation Disorders.
Multiple Pathological Ocular Findings in a Patient With PHACE Syndrome.
📚 EuropePMC10 artigos no totalmostrando 5
Congenital oculomotor nerve palsy with aberrant eyelid movements and pupillary spasms: a case report.
BMC ophthalmologyA modified technique for attaching the lateral rectus muscle to the orbital periosteum through a skin incision over the lateral orbital rim.
Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and StrabismusMagnetic Resonance Imaging in 14 Patients with Congenital Oculomotor Nerve Palsy.
Clinical neuroradiologyImaging of Cranial Nerves III, IV, VI in Congenital Cranial Dysinnervation Disorders.
Korean journal of ophthalmology : KJOMultiple Pathological Ocular Findings in a Patient With PHACE Syndrome.
Journal of pediatric ophthalmology and strabismusAssociações
Organizações que acompanham esta doença — pra ter apoio e orientação
Ainda não temos associações cadastradas para Paralisia congênita do nervo oculomotor.
É de uma associação que acompanha esta doença? Fale com a gente →
Comunidades
Grupos ativos de quem convive com esta doença aqui no Raras
Ainda não existe comunidade no Raras para Paralisia congênita do nervo oculomotor
Pacientes, familiares e cuidadores se organizam em comunidades pra compartilhar experiências, fazer perguntas e se apoiar. Você pode ser o primeiro.
Tire suas dúvidas
Perguntas, dicas e experiências compartilhadas aqui na página
Participe da discussão
Faça login para postar dúvidas, compartilhar experiências e interagir com especialistas.
Fazer loginDoenças relacionadas
Doenças com sintomas parecidos — ajudam quem ainda está buscando diagnóstico
Ainda não achamos doenças com sintomas parecidos o suficiente.
Referências e fontes
Bases de dados externas citadas neste artigo
Publicações científicas
Artigos indexados no PubMed ligados a esta doença no grafo RarasNet — título, periódico e PMID direto da fonte, sem intermediação de IA.
- Congenital oculomotor nerve palsy with aberrant eyelid movements and pupillary spasms: a case report.
- Magnetic Resonance Imaging in 14 Patients with Congenital Oculomotor Nerve Palsy.
- A modified technique for attaching the lateral rectus muscle to the orbital periosteum through a skin incision over the lateral orbital rim.Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus· 2019· PMID 31103564mais citado
- Imaging of Cranial Nerves III, IV, VI in Congenital Cranial Dysinnervation Disorders.
- Multiple Pathological Ocular Findings in a Patient With PHACE Syndrome.
Bases de dados e fontes oficiais
Identificadores e referências canônicas usadas para montar este verbete.
- ORPHA:440221(Orphanet)
- MONDO:0018599(MONDO)
- GARD:21836(GARD (NIH))
- Busca completa no PubMed(PubMed)
- Q55788206(Wikidata)
Dados compilados pelo RarasNet a partir de fontes abertas (Orphanet, OMIM, MONDO, PubMed/EuropePMC, ClinicalTrials.gov, DATASUS, PCDT/MS). Este conteúdo é informativo e não substitui avaliação médica.
Conteúdo mantido por Agente Raras · Médicos e pesquisadores podem colaborar
Paralisia congênita do nervo oculomotor
📋 Origem dos dados
Esta página agrega dados de fontes públicas e oficiais. Dados sobre cobertura no SUS (PCDT, CEAF) são verificados ativamente por agente proativo (ver badge no infobox). Demais dados têm atribuição de fonte + data da última sincronização — clique para abrir o original.
- Doença rara (ontologia)
- fonte: Orphanet
- Identificador unificado
- fonte: MONDO
- Codificação WHO/SUS
- fonte: WHO ICD-10 / DATASUS
- CID-11 (futuro)
- fonte: WHO ICD-11
- NIH/GARD
- fonte: GARD (NIH)
- Dado público estruturado
- fonte: Wikidata