O átrio é uma das duas câmaras superiores do coração que recebe sangue do sistema circulatório. O sangue nos átrios é bombeado para os ventrículos cardíacos através das válvulas cardíacas atrioventriculares mitral e tricúspide.
Introdução
O que você precisa saber de cara
Visão geral
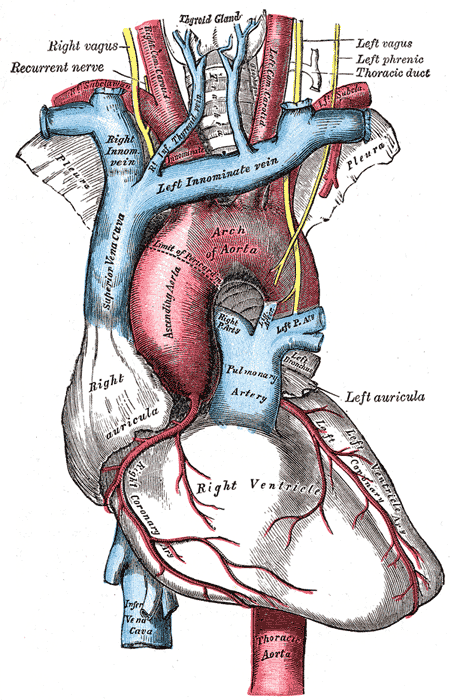
A 'Veia cava superior, direita, ligando ao lado esquerdo da aurícula' é uma malformação vascular congênita rara, na qual a veia cava superior direita (o principal vaso que traz o sangue da cabeça, pescoço e membros superiores de volta ao coração) se conecta anormalmente ao átrio esquerdo, em vez do átrio direito. Isso cria um desvio (shunt) de sangue venoso para o lado esquerdo do coração, causando uma mistura de sangue rico e pobre em oxigênio.[1]
Sinais e sintomas
Os sintomas decorrem principalmente do shunt venoso sistêmico da direita para a esquerda, que leva à hipoxemia arterial (baixo oxigênio no sangue). As manifestações podem incluir cianose (coloração azulada da pele e mucosas), falta de ar aos esforços (dispneia de exercício), baqueteamento digital (alargamento das pontas dos dedos), palpitações e sopros cardíacos. Em casos mais graves, pode ocorrer abscesso cerebral, uma complicação potencialmente fatal.[1]
Causas genéticas
Diagnóstico
O diagnóstico é baseado em exames de imagem cardíaca (como ecocardiograma, angiotomografia ou ressonância magnética) que demonstram a conexão anômala da veia cava superior direita ao átrio esquerdo. Exames genéticos podem ser solicitados para investigar possíveis síndromes associadas, embora não exista um teste genético específico para esta malformação isolada. No âmbito do SUS, estão disponíveis procedimentos como cariótipo, pesquisa de microdeleções por FISH, sequenciamento completo do exoma (WES) e dosagem de alfa-fetoproteína, além de atendimento em reabilitação para doenças raras.[1]
Tratamento e manejo
O tratamento é individualizado e geralmente cirúrgico, visando redirecionar o fluxo da veia cava superior para o átrio direito. O manejo inclui acompanhamento multidisciplinar com cardiologista, cirurgião cardiovascular e geneticista. Não há medicamentos específicos aprovados para tratar a malformação em si; o uso de medicamentos é voltado para o controle de sintomas ou complicações (como antibióticos para profilaxia de abscesso cerebral).[1]
Prognóstico e qualidade de vida
O prognóstico depende da gravidade do shunt e da presença de outras anomalias cardíacas associadas. Com correção cirúrgica adequada, muitos pacientes apresentam melhora significativa da oxigenação e dos sintomas. Sem tratamento, o risco de complicações como abscesso cerebral e insuficiência cardíaca é elevado. O acompanhamento regular é essencial para monitorar a função cardíaca e prevenir eventos adversos.[1]
Conteúdo informativo gerado e mantido automaticamente a partir de fontes oficiais (Orphanet, HPO, OMIM, SUS). Não substitui avaliação médica.
O átrio é uma das duas câmaras superiores do coração que recebe sangue do sistema circulatório. O sangue nos átrios é bombeado para os ventrículos cardíacos através das válvulas cardíacas atrioventriculares mitral e tricúspide.
Encontrou um erro ou informação desatualizada? Sugira uma correção →
Entender a doença
Do básico ao detalhe, leia no seu ritmo
Preparando trilha educativa...
Sinais e sintomas
O que aparece no corpo e com que frequência cada sintoma acontece
Visão geral
A 'Veia cava superior, direita, ligando ao lado esquerdo da aurícula' é uma malformação vascular congênita rara, na qual a veia cava superior direita (o principal vaso que traz o sangue da cabeça, pescoço e membros superiores de volta ao coração) se conecta anormalmente ao átrio esquerdo, em vez do átrio direito. Isso cria um desvio (shunt) de sangue venoso para o lado esquerdo do coração, causando uma mistura de sangue rico e pobre em oxigênio.[1]
Sinais e sintomas
Os sintomas decorrem principalmente do shunt venoso sistêmico da direita para a esquerda, que leva à hipoxemia arterial (baixo oxigênio no sangue). As manifestações podem incluir cianose (coloração azulada da pele e mucosas), falta de ar aos esforços (dispneia de exercício), baqueteamento digital (alargamento das pontas dos dedos), palpitações e sopros cardíacos. Em casos mais graves, pode ocorrer abscesso cerebral, uma complicação potencialmente fatal.[1]
Causas genéticas
Diagnóstico
O diagnóstico é baseado em exames de imagem cardíaca (como ecocardiograma, angiotomografia ou ressonância magnética) que demonstram a conexão anômala da veia cava superior direita ao átrio esquerdo. Exames genéticos podem ser solicitados para investigar possíveis síndromes associadas, embora não exista um teste genético específico para esta malformação isolada. No âmbito do SUS, estão disponíveis procedimentos como cariótipo, pesquisa de microdeleções por FISH, sequenciamento completo do exoma (WES) e dosagem de alfa-fetoproteína, além de atendimento em reabilitação para doenças raras.[1]
Tratamento e manejo
O tratamento é individualizado e geralmente cirúrgico, visando redirecionar o fluxo da veia cava superior para o átrio direito. O manejo inclui acompanhamento multidisciplinar com cardiologista, cirurgião cardiovascular e geneticista. Não há medicamentos específicos aprovados para tratar a malformação em si; o uso de medicamentos é voltado para o controle de sintomas ou complicações (como antibióticos para profilaxia de abscesso cerebral).[1]
Prognóstico e qualidade de vida
O prognóstico depende da gravidade do shunt e da presença de outras anomalias cardíacas associadas. Com correção cirúrgica adequada, muitos pacientes apresentam melhora significativa da oxigenação e dos sintomas. Sem tratamento, o risco de complicações como abscesso cerebral e insuficiência cardíaca é elevado. O acompanhamento regular é essencial para monitorar a função cardíaca e prevenir eventos adversos.[1]
Conteúdo informativo gerado e mantido automaticamente a partir de fontes oficiais (Orphanet, HPO, OMIM, SUS). Não substitui avaliação médica.
Linha do tempo da pesquisa
Encontrou um erro ou informação desatualizada? Sugira uma correção →
Genética e causas
O que está alterado no DNA e como passa nas famílias
Nenhum gene associado encontrado
Os dados genéticos desta condição ainda estão sendo catalogados.
Diagnóstico
Os sinais que médicos procuram e os exames que confirmam
Tratamento e manejo
Remédios, cuidados de apoio e o que precisa acompanhar
Onde tratar no SUS
Hospitais de referência no Brasil e o protocolo oficial do SUS (PCDT)
🇧🇷 Atendimento SUS — Veia cava superior, direita, ligando ao lado esquerdo da aurícula
Selecione um estado ou use sua localização para ver resultados.
Dados de DATASUS/CNES, SBGM, ABNeuro e Ministério da Saúde. Sempre confirme a disponibilidade diretamente com o estabelecimento.
Pesquisa ativa
Ensaios clínicos abertos e novidades científicas recentes
Pesquisa e ensaios clínicos
Nenhum ensaio clínico registrado para esta condição.
Publicações mais relevantes
Double superior vena cava and anomalous left atrial drainage of persistent left SVC: A case report.
Persistent left superior vena cava (PLSVC) is an uncommon developmental variation of the thoracic venous system, sometimes accompanied by a duplicated superior vena cava (SVC). While often asymptomatic when draining into the right atrium, drainage toward the left atrium could lead to a right-to-left shunt and potential compromise of whole-body oxygen delivery. This report describes a 48-year-old male patient with hypertension and chronic tobacco use who was evaluated for dyspnea and leg edema. Imaging revealed a double SVC, where the left-sided vessel connected directly to the left atrium. Despite this anomaly, the patient exhibited no significant hypoxemia or cyanosis, likely due to long-term compensatory mechanisms. This report underscores the need to consider vascular anomalies in imaging interpretation, particularly when findings are incidental. It also underscores the role of contrast-enhanced CT in identifying rare anatomical variants and the potential for such anomalies to remain clinically silent despite physiological significance.
Chylothorax after patent ductus arteriosus ligation in a dog with persistent left cranial vena cava.
This report is the first to document chylothorax after patent ductus arteriosus (PDA) ligation in a dog with a persistent left cranial vena cava (PLCVC), highlighting potential complications arising from concurrent cardiovascular anomalies. A nine-month-old female desexed Pomeranian was referred for PDA. Echocardiography confirmed a left-to-right shunt with mild left-sided cardiac changes from volume overload. At left fourth intercostal thoracotomy, an aberrant vein (5 mm) coursing over the PDA within the mediastinum was retracted proximally to facilitate PDA ligation. Retraction was released before thoracotomy closure, and the vein remained grossly unaltered. The dog represented 3 days postoperative for dyspnoea and had bilateral chylous pleural effusion. Thoracic computed tomography with intravenous contrast identified a complete PLCVC, which was continuous with the left brachiocephalic vein and inserted into the right atrium without any venous connection to the normal right cranial vena cava. A thoracostomy tube was placed, and the chylothorax resolved spontaneously. Repeat echocardiogram eight weeks postoperative showed normal laminar trans-pulmonic flow and reversal of cardiac changes. It is hypothesised that an acute increase in hydrostatic venous pressure from transient obstruction of the PLCVC during intraoperative retraction impeded thoracic duct emptying into the venous system. This in turn may have caused chyle leakage through afferent lymphatics with chylothorax. It is unlikely PLCVC thrombosis was a cause given chylothorax was transient and the PLCVC was normal on computed tomography (CT); nor iatrogenic thoracic duct damage given the surgical approach was left-sided and the duct courses through the right.
Surgical correction of total anomalous pulmonary venous connection to persistent left-sided superior vena cava: a case report.
Total anomalous pulmonary venous connection (TAPVC) to left superior vena cava (LSVC) is an extremely rare congenital heart disease, and its surgical management is very challenging. We report one such case of a 5-year-old south Asian male with double outlet right ventricle and unbalanced atrioventricular canal defect, where all the pulmonary veins were found opening into LSVC, which was then opening into the left side of the common atrium. Intraoperatively, the LSVC was transected just below the left internal jugular vein and left subclavian vein junction and left-sided bidirectional Glenn shunt done using 8 mm Dacron tube graft. Pulmonary veins were left draining through the LSVC into the common atrium. Right-sided Glenn shunt was completed as usual. Currently, the patient is year and half post-surgery and is doing well; school going on par with the peer group maintaining a room air saturation of 87%. Here, we report a successful surgical correction of TAPVC to LSVC in a child with univentricular physiology, however due to the paucity of data and rarity of such cases, optimal surgical management is yet to be defined.
TAPVR: Molecular Pathways and Animal Models.
The venous pole of the heart where the pulmonary veins will develop encompasses the sinus venosus and the atrium. In the fourth week of development, the sinus venosus consists of a left and a right part receiving blood from the common cardinal vein, the omphalomesenteric and umbilical veins. Asymmetrical expansion of the common atrium corresponds with a rightward shift of the connection of the sinus to the atrium. The right-sided part of the sinus venosus including its tributing cardinal veins enlarges to form the right superior and inferior vena cava that will incorporate into the right atrium. The left-sided part in human development largely obliterates and remodels to form the coronary sinus in adults. In approximately the same time window (4th-fifth weeks), a splanchnic vascular plexus surrounds the developing lung buds (putative lungs) with a twofold connection. Of note, during early developmental stages, the primary route of drainage from the pulmonary plexus is toward the systemic veins and not to the heart. After lumenization of the so-called mid-pharyngeal endothelial strand (MPES), the first anlage of the pulmonary vein, the common pulmonary vein can be observed in the dorsal mesocardium, and the primary route of drainage will gradually change toward a cardiac drainage. The splanchnic pulmonary venous connections with the systemic cardinal veins will gradually disappear during normal development. In case of absence or atresia of the MPES, the pulmonary-to-systemic connections will persist, clinically resulting in total anomalous pulmonary venous return (TAPVR). This chapter describes the developmental processes and molecular pathways underlying anomalous pulmonary venous connections. The inferior vena cava (IVC) is a large retroperitoneal vessel formed by the confluence of the right and left common iliac veins. Anatomically this usually occurs at the L5 vertebral level. The IVC lies along the right anterolateral aspect of the vertebral column and passes through the central tendon of the diaphragm around the T8 vertebral level. The IVC is a large blood vessel responsible for transporting deoxygenated blood from the lower extremities and abdomen back to the right atrium of the heart. It has the largest diameter of the venous system and is a thin-walled vessel. These anatomic characteristics make it ideal for transporting large quantities of venous blood. Many veins contain one-way valves to ensure the forward flow of blood back toward the heart. The IVC, however, does not contain such valves, and forward flow to the heart is driven by the differential pressure created by normal respiration. As the diaphragm contracts and creates negative pressure in the chest for the lungs to fill with air, this pressure gradient pulls the venous blood from the abdominal IVC into the thoracic IVC and subsequently into the right heart. The IVC enters the right atrium of the heart after coursing through the diaphragm, entering the posterior inferior aspect of the atrium. The IVC enters the right atrium inferior to the entrance of the superior vena cava (SVC). The IVC is a mostly symmetric vessel with a few exceptions. Due to the IVC residing on the right side of the vertebral column the vessels entering the IVC from the left side of the body, like the left renal vein, are longer than their anatomic counterparts on the right. Other left-sided veins, like the left adrenal and left gonadal vein, first join the left renal vein before joining the IVC and continuing as venous flow returning to the heart. This differs from the right side of the body where the right adrenal and right gonadal vein directly join the IVC without first joining the right renal vein. Anatomic variants venous of anatomy involving both right and left sides have been described. Blood from the left and right femoral veins enters the IVC via the left and right common iliac veins, respectively. Blood from the abdominal viscera travels into the portal vein and enters the IVC via the hepatic veins after traversing the liver and its sinusoids. Venous blood from the abdominal wall reaches the IVC through lumbar veins. Ascending lumbar veins connect lumbar veins to the azygos vein and this provides some collateral circulation between the inferior vena cava and the superior vena cava. This potential for a collateral flow could be critical if either of the larger veins becomes obstructed. Below is a list of (most common) vertebral levels at which different veins enter the IVC. T8: Hepatic veins, inferior phrenic veins . L1: Right suprarenal vein, renal veins . L2: Right gonadal vein . L1-L5: Lumbar vertebral veins . L5: Right and left common iliac veins.
Partial Anomalous Pulmonary Venous Connection With Intact Atrial Septum: Early and Midterm Outcomes.
Partial anomalous pulmonary venous return with intact atrial septum warrants greater understanding and evaluation in the literature. From January 1993 to December 2018, 293 patients with partial anomalous pulmonary venous return underwent surgical repair. Of these, 45 patients (15.3%) had an intact atrial septum. The median age was 36 years (interquartile range, 24-48). Direct reimplantation was used in 17 patients (38%), intracardiac baffling in 15 (33%), and caval division (Warden) technique in 13 (29%). Descriptive statistics were used to assess the data, and Kaplan-Meier analysis was used to assess survival. Anomalous veins were right-sided in 27 patients (60%), left-sided in 16 patients (36%), and bilateral in 2 patients (4%). The insertion sites were the superior vena cava in 23 patients (51%), innominate vein in 12 (27%), inferior vena cava in 6 (13%), coronary sinus in 2 (4%), right atrium in 1 patient (2%), and unknown in 1 patient (2%). Scimitar syndrome was noted in 8 patients (18%). There was no postoperative mortality or residual defects. Postoperative echocardiography excluded any obstruction of pulmonary or systemic veins. Postoperative complications included atrial fibrillation in 9 patients (20%) and pneumothorax requiring chest tube in 5 patients (11%). Survival at 1, 5, and 10 years was 100%, 95%, and 95%, respectively. Two patients underwent pulmonary vein dilation, one at 3 years and the other at 7 years. Surgical repair of partial anomalous pulmonary venous connection with intact atrial septum can be performed with excellent early and midterm outcomes. The overall incidence of midterm systemic or pulmonary vein stenosis is low.
Publicações recentes
Partial Anomalous Pulmonary Venous Connection With Intact Atrial Septum: Early and Midterm Outcomes.
Heart Transplant in Patient With Isolated Left Superior Vena Cava by Atrial Appendage Rotation.
Prenatal diagnosis of isolated total anomalous systemic venous connection to the left atrium.
Variants of the scimitar syndrome.
Myocardium of the superior vena cava, coronary sinus, vein of Marshall, and the pulmonary vein ostia: gross anatomic studies in 620 hearts.
📚 EuropePMCmostrando 14
Double superior vena cava and anomalous left atrial drainage of persistent left SVC: A case report.
Radiology case reportsChylothorax after patent ductus arteriosus ligation in a dog with persistent left cranial vena cava.
Australian veterinary journalSurgical correction of total anomalous pulmonary venous connection to persistent left-sided superior vena cava: a case report.
European heart journal. Case reportsTAPVR: Molecular Pathways and Animal Models.
Advances in experimental medicine and biologyPartial Anomalous Pulmonary Venous Connection With Intact Atrial Septum: Early and Midterm Outcomes.
The Annals of thoracic surgeryAtretic Coronary Sinus Orifice and a Diverticulum of Coronary Sinus Associated with Persistent Left Superior Vena Cava and Accessory Pathway.
Journal of cardiovascular echographyNeonatal intra-atrial baffle repair for isolated ventricular inversion with left isomerism: a case report.
Surgical case reportsCongenital systemic venous return anomalies to the right atrium review.
Insights into imagingRobotic repair of partial anomalous pulmonary venous connection: the initial experience and technical details.
Journal of robotic surgeryHeart Transplant in Patient With Isolated Left Superior Vena Cava by Atrial Appendage Rotation.
The Annals of thoracic surgeryLow-Dose Computed Tomographic Imaging of Partial Anomalous Pulmonary Venous Connection in Children.
World journal for pediatric & congenital heart surgeryPrenatal diagnosis of isolated total anomalous systemic venous connection to the left atrium.
Cardiology in the youngOutcome after surgical repair of partial anomalous pulmonary venous connection.
Pakistan journal of medical sciencesVariants of the scimitar syndrome.
Cardiology in the youngAssociações
Organizações que acompanham esta doença — pra ter apoio e orientação
Ainda não temos associações cadastradas para Veia cava superior, direita, ligando ao lado esquerdo da aurícula.
É de uma associação que acompanha esta doença? Fale com a gente →
Comunidades
Grupos ativos de quem convive com esta doença aqui no Raras
Ainda não existe comunidade no Raras para Veia cava superior, direita, ligando ao lado esquerdo da aurícula
Pacientes, familiares e cuidadores se organizam em comunidades pra compartilhar experiências, fazer perguntas e se apoiar. Você pode ser o primeiro.
Tire suas dúvidas
Perguntas, dicas e experiências compartilhadas aqui na página
Participe da discussão
Faça login para postar dúvidas, compartilhar experiências e interagir com especialistas.
Fazer loginDoenças relacionadas
Doenças com sintomas parecidos — ajudam quem ainda está buscando diagnóstico
Ainda não achamos doenças com sintomas parecidos o suficiente.
Referências e fontes
Bases de dados externas citadas neste artigo
Publicações científicas
Artigos indexados no PubMed ligados a esta doença no grafo RarasNet — título, periódico e PMID direto da fonte, sem intermediação de IA.
- Double superior vena cava and anomalous left atrial drainage of persistent left SVC: A case report.
- Chylothorax after patent ductus arteriosus ligation in a dog with persistent left cranial vena cava.
- Surgical correction of total anomalous pulmonary venous connection to persistent left-sided superior vena cava: a case report.
- TAPVR: Molecular Pathways and Animal Models.
- Partial Anomalous Pulmonary Venous Connection With Intact Atrial Septum: Early and Midterm Outcomes.
- Heart Transplant in Patient With Isolated Left Superior Vena Cava by Atrial Appendage Rotation.
- Prenatal diagnosis of isolated total anomalous systemic venous connection to the left atrium.
- Variants of the scimitar syndrome.
- Myocardium of the superior vena cava, coronary sinus, vein of Marshall, and the pulmonary vein ostia: gross anatomic studies in 620 hearts.
Bases de dados e fontes oficiais
Identificadores e referências canônicas usadas para montar este verbete.
- ORPHA:99110(Orphanet)
- MONDO:0020441(MONDO)
- GARD:19653(GARD (NIH))
- Busca completa no PubMed(PubMed)
- Q55789374(Wikidata)
Dados compilados pelo RarasNet a partir de fontes abertas (Orphanet, OMIM, MONDO, PubMed/EuropePMC, ClinicalTrials.gov, DATASUS, PCDT/MS). Este conteúdo é informativo e não substitui avaliação médica.
Conteúdo mantido por Agente Raras · Médicos e pesquisadores podem colaborar
Veia cava superior, direita, ligando ao lado esquerdo da aurícula
📋 Origem dos dados
Esta página agrega dados de fontes públicas e oficiais. Dados sobre cobertura no SUS (PCDT, CEAF) são verificados ativamente por agente proativo (ver badge no infobox). Demais dados têm atribuição de fonte + data da última sincronização — clique para abrir o original.
- Doença rara (ontologia)
- fonte: Orphanet
- Identificador unificado
- fonte: MONDO
- Codificação WHO/SUS
- fonte: WHO ICD-10 / DATASUS
- CID-11 (futuro)
- fonte: WHO ICD-11
- NIH/GARD
- fonte: GARD (NIH)
- Dado público estruturado
- fonte: Wikidata