É uma doença muscular rara e genética, transmitida por um gene dominante, que afeta principalmente os músculos das extremidades do corpo (mãos e pés). Ela causa fraqueza prioritariamente no dedão do pé, nos músculos que levantam a ponta do pé, nos que esticam os dedos das mãos e nos que dobram o pescoço para frente. A progressão da doença é lenta, e há variações na idade em que os sintomas começam a aparecer, na gravidade, no nível de fraqueza e no envolvimento do coração e dos pulmões.
Introdução
O que você precisa saber de cara
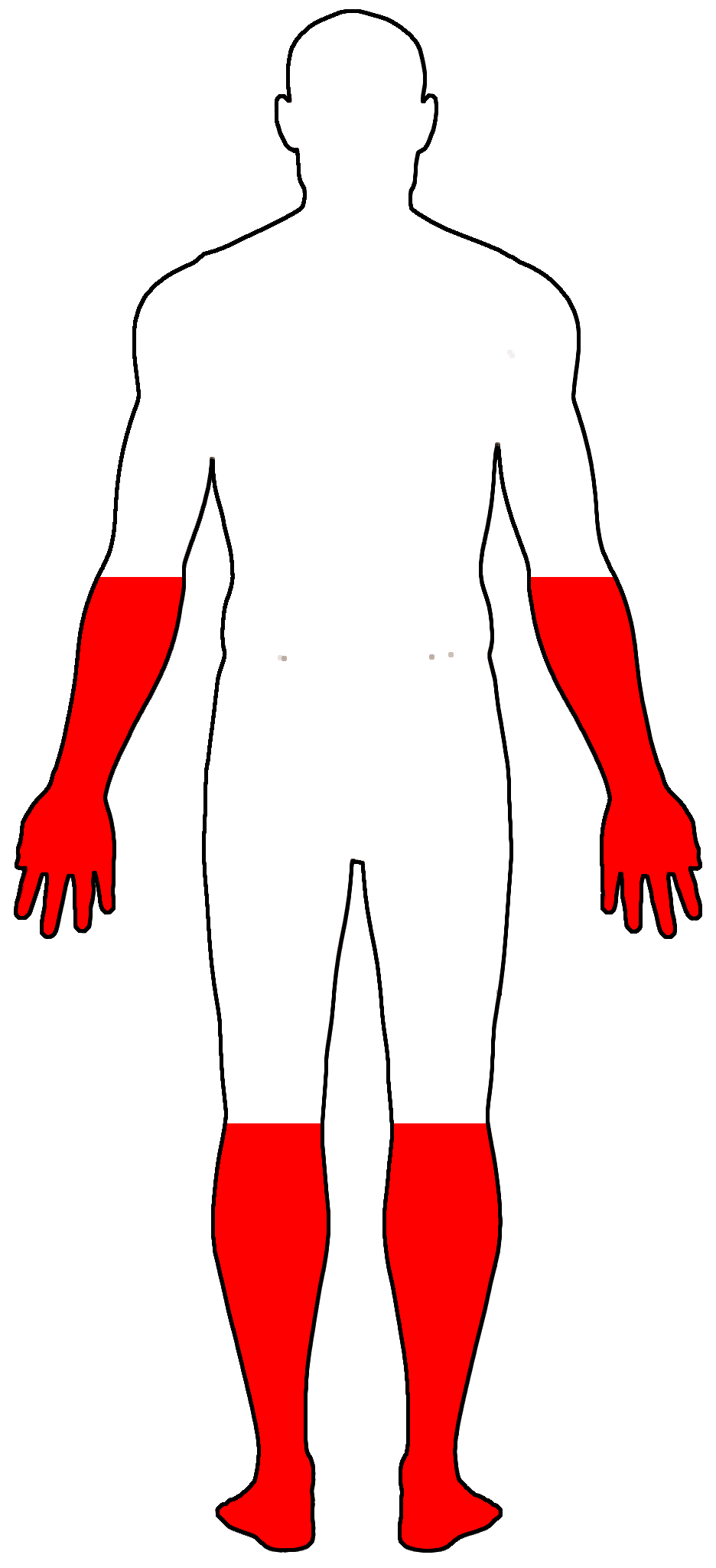
É uma doença muscular rara e genética, transmitida por um gene dominante, que afeta principalmente os músculos das extremidades do corpo (mãos e pés). Ela causa fraqueza prioritariamente no dedão do pé, nos músculos que levantam a ponta do pé, nos que esticam os dedos das mãos e nos que dobram o pescoço para frente. A progressão da doença é lenta, e há variações na idade em que os sintomas começam a aparecer, na gravidade, no nível de fraqueza e no envolvimento do coração e dos pulmões.
Escala de raridade
<1/50kMuito rara
1/20kRara
1/10kPouco freq.
1/5kIncomum
1/2k
Encontrou um erro ou informação desatualizada? Sugira uma correção →
Entender a doença
Do básico ao detalhe, leia no seu ritmo
Preparando trilha educativa...
Sinais e sintomas
O que aparece no corpo e com que frequência cada sintoma acontece
Partes do corpo afetadas
+ 10 sintomas em outras categorias
Características mais comuns
Os sintomas variam de pessoa para pessoa. Abaixo estão as 38 características clínicas mais associadas, ordenadas por frequência.
Linha do tempo da pesquisa
Encontrou um erro ou informação desatualizada? Sugira uma correção →
Genética e causas
O que está alterado no DNA e como passa nas famílias
Genes associados
1 gene identificado com associação a esta condição. Padrão de herança: Autosomal dominant.
Curadoria gene-doença
fontes oficiaisMyosins are actin-based motor molecules with ATPase activity essential for muscle contraction. Forms regular bipolar thick filaments that, together with actin thin filaments, constitute the fundamental contractile unit of skeletal and cardiac muscle
Cytoplasm, myofibrilCytoplasm, myofibril, sarcomere
Cardiomyopathy, familial hypertrophic, 1
A hereditary heart disorder characterized by ventricular hypertrophy, which is usually asymmetric and often involves the interventricular septum. The symptoms include dyspnea, syncope, collapse, palpitations, and chest pain. They can be readily provoked by exercise. The disorder has inter- and intrafamilial variability ranging from benign to malignant forms with high risk of cardiac failure and sudden cardiac death.
Variantes genéticas (ClinVar)
1.439 variantes patogênicas registradas no ClinVar.
Diagnóstico
Os sinais que médicos procuram e os exames que confirmam
Tratamento e manejo
Remédios, cuidados de apoio e o que precisa acompanhar
Onde tratar no SUS
Hospitais de referência no Brasil e o protocolo oficial do SUS (PCDT)
🇧🇷 Atendimento SUS — Miopatia distal Laing
Selecione um estado ou use sua localização para ver resultados.
Dados de DATASUS/CNES, SBGM, ABNeuro e Ministério da Saúde. Sempre confirme a disponibilidade diretamente com o estabelecimento.
Pesquisa ativa
Ensaios clínicos abertos e novidades científicas recentes
Pesquisa e ensaios clínicos
Nenhum ensaio clínico registrado para esta condição.
Publicações mais relevantes
Generation of iPSC lines from three Laing distal myopathy patients with a recurrent MYH7 p.Lys1617del variant.
Variants in MYH7 cause cardiomyopathies as well as myosin storage myopathy and Laing early-onset distal myopathy (MPD1). MPD1 is characterized by muscle weakness and atrophy usually beginning in the lower legs. Here, we generated iPSC lines from lymphoblastoid cells of three unrelated individuals heterozygous for the most common MPD1-causing variant; p.Lys1617del. iPSC lines showed typical morphology, expressed pluripotency markers, demonstrated trilineage differentiation potential, and had a normal karyotype. These lines represent the first iPSCs derived from MPD1 patients and complement existing MPD1 animal models. They can provide in vitro platforms to better understand and model MPD1 pathomechanisms and test therapies.
A therapeutic leap: how myosin inhibitors moved from cardiac interventions to skeletal muscle myopathy solutions.
The myosin inhibitor mavacamten has transformed the management of obstructive hypertrophic cardiomyopathy (HCM) by targeting myosin ATPase activity to mitigate cardiac hypercontractility. This therapeutic mechanism has proven effective for patients with HCM independent of having a primary gene mutation in myosin. In this issue of the JCI, Buvoli et al. report that muscle hypercontractility is a mechanism of pathogenesis underlying muscle dysfunction in Laing distal myopathy, a disorder characterized by mutations altering the rod domain of β myosin heavy chain. The authors performed detailed physiological, molecular, and biomechanical analyses and demonstrated that myosin ATPase inhibition can correct a large extent of muscle abnormalities. The findings offer a therapeutic avenue for Laing distal myopathy and potentially other myopathies. This Commentary underscores the importance of reevaluating myosin activity's role across myopathies in general for the potential development of targeted myosin inhibitors to treat skeletal muscle disorders.
A Laing distal myopathy-associated proline substitution in the β-myosin rod perturbs myosin cross-bridging activity.
Proline substitutions within the coiled-coil rod region of the β-myosin gene (MYH7) are the predominant mutations causing Laing distal myopathy (MPD1), an autosomal dominant disorder characterized by progressive weakness of distal/proximal muscles. We report that the MDP1 mutation R1500P, studied in what we believe to be the first mouse model for the disease, adversely affected myosin motor activity despite being in the structural rod domain that directs thick filament assembly. Contractility experiments carried out on isolated mutant muscles, myofibrils, and myofibers identified muscle fatigue and weakness phenotypes, an increased rate of actin-myosin detachment, and a conformational shift of the myosin heads toward the more reactive disordered relaxed (DRX) state, causing hypercontractility and greater ATP consumption. Similarly, molecular analysis of muscle biopsies from patients with MPD1 revealed a significant increase in sarcomeric DRX content, as observed in a subset of myosin motor domain mutations causing hypertrophic cardiomyopathy. Finally, oral administration of MYK-581, a small molecule that decreases the population of heads in the DRX configuration, significantly improved the limited running capacity of the R1500P-transgenic mice and corrected the increased DRX state of the myofibrils from patients. These studies provide evidence of the molecular pathogenesis of proline rod mutations and lay the groundwork for the therapeutic advancement of myosin modulators.
A case report of deglutition triggered atrial fibrillation in a patient with Laing distal myopathy.
Deglutition-induced atrial fibrillation is a rare clinical entity with a reported prevalence of 0.6%. Laing distal myopathy is a rare autosomal dominant muscular dystrophy that is the result of mutations within the slow skeletal muscle fibre myosin heavy chain gene (MYH7). Atrial fibrillation has not been previously reported in patients with Laing distal myopathy. We describe the first reported case of deglutition triggered atrial fibrillation in a female with a history of Laing distal myopathy. A 44-year-old female with a history of Laing distal myopathy diagnosed at age 32, began experiencing intermittent episodes of pre-syncope and palpitations which occurred after deglutition with food. An ambulatory 30-day patient triggered event monitor recorded episodes of atrial fibrillation with rapid ventricular response. Family history was significant for Laing distal myopathy, atrial fibrillation, as well as sudden cardiac death. Laboratory data, transthoracic echocardiogram, cardiac magnetic resonance imaging, and an exercise treadmill SPECT Imaging stress test were normal. An oesophagram revealed a mild oesophageal dysmotility with no other abnormalities. She was started on flecainide 50 mg p.o. every 8 h and verapamil 40 mg p.o. every 8 h with no further episodes of atrial fibrillation. Given the strong genetic component of this myopathy, one could postulate as to a possible genetic component in the development of atrial fibrillation in our patient. Although we cannot make definite correlation between deglutition-induced atrial fibrillation and Laing myopathy, it is important to report this unusual association which has not been described before.
A study of the phenotypic variability and disease progression in Laing myopathy through the evaluation of muscle imaging.
Laing myopathy is characterized by broad clinical and pathological variability. They are limited in number and protocol of study. We aimed to delineate muscle imaging profiles and validate imaging analysis as an outcome measure. This was a cross-sectional and longitudinal cohort study. Data from clinical, functional and semi-quantitative muscle imaging (60 magnetic resonance imaging [MRI] and six computed tomography scans) were studied. Hierarchical analysis, graphic heatmap representation and correlation between imaging and clinical data using Bayesian statistics were carried out. The study cohort comprised 42 patients from 13 families harbouring five MYH7 mutations. The cohort had a wide range of ages, age at onset, disease duration, and myopathy extension and Gardner-Medwin and Walton (GMW) functional scores. Intramuscular fat was evident in all but two asymptomatic/pauci-symptomatic patients. Anterior leg compartment muscles were the only affected muscles in 12% of the patients. Widespread extension to the thigh, hip, paravertebral and calf muscles and, less frequently, the scapulohumeral muscles was commonly observed, depicting distinct patterns and rates of progression. Foot muscles were involved in 40% of patients, evolving in parallel to other regions with absence of a disto-proximal gradient. Whole cumulative imaging score, ranging from 0 to 2.9 out of 4, was associated with disease duration and with myopathy extension and GMW scales. Follow-up MRI studies in 24 patients showed significant score progression at a variable rate. We confirmed that the anterior leg compartment is systematically affected in Laing myopathy and may represent the only manifestation of this disorder. However, widespread muscle involvement in preferential but variable and not distance-dependent patterns was frequently observed. Imaging score analysis is useful to categorize patients and to follow disease progression over time.
Publicações recentes
Generation of iPSC lines from three Laing distal myopathy patients with a recurrent MYH7 p.Lys1617del variant.
A therapeutic leap: how myosin inhibitors moved from cardiac interventions to skeletal muscle myopathy solutions.
A Laing distal myopathy-associated proline substitution in the β-myosin rod perturbs myosin cross-bridging activity.
A case report of deglutition triggered atrial fibrillation in a patient with Laing distal myopathy.
MYH7-related disorders in two Bulgarian families: Novel variants in the same region associated with different clinical manifestation and disease penetrance.
📚 EuropePMC17 artigos no totalmostrando 21
Generation of iPSC lines from three Laing distal myopathy patients with a recurrent MYH7 p.Lys1617del variant.
Stem cell researchA therapeutic leap: how myosin inhibitors moved from cardiac interventions to skeletal muscle myopathy solutions.
The Journal of clinical investigationA Laing distal myopathy-associated proline substitution in the β-myosin rod perturbs myosin cross-bridging activity.
The Journal of clinical investigationA case report of deglutition triggered atrial fibrillation in a patient with Laing distal myopathy.
European heart journal. Case reportsMYH7-related disorders in two Bulgarian families: Novel variants in the same region associated with different clinical manifestation and disease penetrance.
Neuromuscular disorders : NMDClinical features and genotypes of Laing distal myopathy in a group of Chinese patients, with in-frame deletions of MYH7 as common mutations.
Orphanet journal of rare diseasesA study of the phenotypic variability and disease progression in Laing myopathy through the evaluation of muscle imaging.
European journal of neurologyLaing Myopathy: Report of 4 New Families With Novel MYH7 Mutations, Double Mutations, and Severe Phenotype.
Journal of clinical neuromuscular diseaseA novel MYH7 mutation resulting in Laing distal myopathy in a Chinese family.
Chinese medical journalA novel MYH7 founder mutation causing Laing distal myopathy in Southern Spain.
Neuromuscular disorders : NMDDrosophila model of myosin myopathy rescued by overexpression of a TRIM-protein family member.
Proceedings of the National Academy of Sciences of the United States of AmericaResearch progress of myosin heavy chain genes in human genetic diseases.
Yi chuan = HereditasNovel phenotypic variant in the MYH7 spectrum due to a stop-loss mutation in the C-terminal region: a case report.
BMC medical geneticsTwo novel MYH7 proline substitutions cause Laing Distal Myopathy-like phenotypes with variable expressivity and neck extensor contracture.
BMC medical geneticsLaing distal myopathy with a novel mutation in exon 34 of the MYH7 gene.
Neuromuscular disorders : NMDMYH7-related myopathies: clinical, histopathological and imaging findings in a cohort of Italian patients.
Orphanet journal of rare diseasesDistal myopathy with coexisting heterozygous TIA1 and MYH7 Variants.
Neuromuscular disorders : NMDTwo families with MYH7 distal myopathy associated with cardiomyopathy and core formations.
Journal of clinical neuromuscular diseaseA rare mutation in MYH7 gene occurs with overlapping phenotype.
Biochemical and biophysical research communicationsLaing distal myopathy pathologically resembling inclusion body myositis.
Annals of clinical and translational neurologyA de novo mutation of the MYH7 gene in a large Chinese family with autosomal dominant myopathy.
Human genome variationAssociações
Organizações que acompanham esta doença — pra ter apoio e orientação
Ainda não temos associações cadastradas para Miopatia distal Laing.
É de uma associação que acompanha esta doença? Fale com a gente →
Comunidades
Grupos ativos de quem convive com esta doença aqui no Raras
Ainda não existe comunidade no Raras para Miopatia distal Laing
Pacientes, familiares e cuidadores se organizam em comunidades pra compartilhar experiências, fazer perguntas e se apoiar. Você pode ser o primeiro.
Tire suas dúvidas
Perguntas, dicas e experiências compartilhadas aqui na página
Participe da discussão
Faça login para postar dúvidas, compartilhar experiências e interagir com especialistas.
Fazer loginDoenças relacionadas
Doenças com sintomas parecidos — ajudam quem ainda está buscando diagnóstico
Referências e fontes
Bases de dados externas citadas neste artigo
Publicações científicas
Artigos indexados no PubMed ligados a esta doença no grafo RarasNet — título, periódico e PMID direto da fonte, sem intermediação de IA.
- Generation of iPSC lines from three Laing distal myopathy patients with a recurrent MYH7 p.Lys1617del variant.
- A therapeutic leap: how myosin inhibitors moved from cardiac interventions to skeletal muscle myopathy solutions.
- A Laing distal myopathy-associated proline substitution in the β-myosin rod perturbs myosin cross-bridging activity.
- A case report of deglutition triggered atrial fibrillation in a patient with Laing distal myopathy.
- A study of the phenotypic variability and disease progression in Laing myopathy through the evaluation of muscle imaging.
- MYH7-related disorders in two Bulgarian families: Novel variants in the same region associated with different clinical manifestation and disease penetrance.
Bases de dados e fontes oficiais
Identificadores e referências canônicas usadas para montar este verbete.
- ORPHA:59135(Orphanet)
- OMIM OMIM:160500(OMIM)
- MONDO:0008050(MONDO)
- GARD:10769(GARD (NIH))
- Variantes catalogadas(ClinVar)
- Busca completa no PubMed(PubMed)
- Q3331456(Wikidata)
Dados compilados pelo RarasNet a partir de fontes abertas (Orphanet, OMIM, MONDO, PubMed/EuropePMC, ClinicalTrials.gov, DATASUS, PCDT/MS). Este conteúdo é informativo e não substitui avaliação médica.
Conteúdo mantido por Agente Raras · Médicos e pesquisadores podem colaborar
Miopatia distal Laing
📋 Origem dos dados
Esta página agrega dados de fontes públicas e oficiais. Dados sobre cobertura no SUS (PCDT, CEAF) são verificados ativamente por agente proativo (ver badge no infobox). Demais dados têm atribuição de fonte + data da última sincronização — clique para abrir o original.
- Doença rara (ontologia)
- fonte: Orphanet
- Identificador unificado
- fonte: MONDO
- Genética mendeliana
- fonte: OMIM
- Codificação WHO/SUS
- fonte: WHO ICD-10 / DATASUS
- NIH/GARD
- fonte: GARD (NIH)
- Indexação biomédica
- fonte: MeSH (NLM)
- Dado público estruturado
- fonte: Wikidata