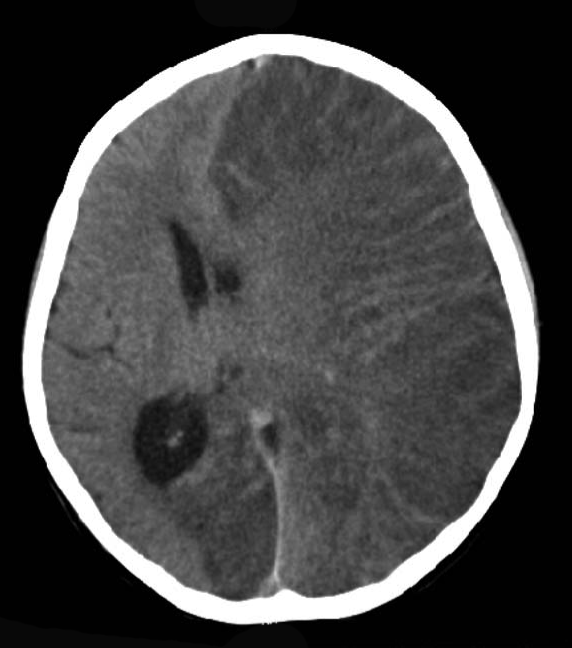
Inflamação crônica rara e progressiva de um único hemisfério cerebral que geralmente afeta crianças. É caracterizada por convulsões graves, perda de habilidades motoras e da fala, hemiparesia e demência.
Introdução
O que você precisa saber de cara
Inflamação crônica rara e progressiva de um único hemisfério cerebral que geralmente afeta crianças. É caracterizada por convulsões graves, perda de habilidades motoras e da fala, hemiparesia e demência.
Escala de raridade
<1/50kMuito rara
1/20kRara
1/10kPouco freq.
1/5kIncomum
1/2k
Encontrou um erro ou informação desatualizada? Sugira uma correção →
Entender a doença
Do básico ao detalhe, leia no seu ritmo
Preparando trilha educativa...
Sinais e sintomas
O que aparece no corpo e com que frequência cada sintoma acontece
Partes do corpo afetadas
+ 17 sintomas em outras categorias
Características mais comuns
Os sintomas variam de pessoa para pessoa. Abaixo estão as 48 características clínicas mais associadas, ordenadas por frequência.
Linha do tempo da pesquisa
Encontrou um erro ou informação desatualizada? Sugira uma correção →
Genética e causas
O que está alterado no DNA e como passa nas famílias
Nenhum gene associado encontrado
Os dados genéticos desta condição ainda estão sendo catalogados.
Diagnóstico
Os sinais que médicos procuram e os exames que confirmam
Tratamento e manejo
Remédios, cuidados de apoio e o que precisa acompanhar
Onde tratar no SUS
Hospitais de referência no Brasil e o protocolo oficial do SUS (PCDT)
🇧🇷 Atendimento SUS — Encefalite subaguda de Rasmussen
Selecione um estado ou use sua localização para ver resultados.
Dados de DATASUS/CNES, SBGM, ABNeuro e Ministério da Saúde. Sempre confirme a disponibilidade diretamente com o estabelecimento.
Pesquisa ativa
Ensaios clínicos abertos e novidades científicas recentes
Ensaios em destaque
🟢 Recrutando agora
1 pesquisa recrutando participantes. Converse com seu médico sobre a possibilidade de participar.
Outros ensaios clínicos
7 ensaios clínicos encontrados, 2 ativos.
Publicações mais relevantes
Bilateral Rasmussen Encephalitis: Good Outcome Following Hemispherotomy.
Bilateral Rasmussen encephalitis is a rare variant of a debilitating, typically unihemispheric disease with limited treatment options. Few cases with bilateral histopathology have been reported, all with poor seizure control following surgery. Here we report a favorable outcome following hemispherotomy in a four-year-old male with biopsy-confirmed bilateral disease. The patient presented with right hemispheric focal seizures with behavioral arrest and over a year progressed to left lower extremity clonic seizures, epilepsia partialis continua, and loss of ambulation, with transient response to steroids and tacrolimus. Histopathology confirmed bilateral disease. The patient developed super-refractory status epilepticus and underwent right functional hemispherotomy 4.5 years after initial presentation. In a 2.5-year follow-up period, an Engel 1D outcome classification was observed with substantially improved quality of life. Previous reports of bilateral Rasmussen encephalitis describe universally poor outcomes, and hemispherotomy is often considered contraindicated. However, hemispherotomy in a patient with bilateral Rasmussen encephalitis may have a good outcome if seizures are unihemispheric.
The Important Role of Hemispherotomy for Rasmussen Encephalitis: Clinical and Functional Outcomes.
Rasmussen encephalitis (RE) is characterized by pharmacoresistant epilepsy and progressive neurological deficits concurrent with unilateral hemispheric atrophy. Evidence of an inflammatory autoimmune process has been extensively described in the literature; however, the precise etiology of RE is still unknown. Despite data supporting a beneficial effect of early immunosuppressive and immunomodulatory interventions, surgical disconnection of the affected hemisphere is considered the treatment of choice for these patients. The aim of this study was to report a series of children and adolescents who underwent hemispheric surgery (HS) for the treatment of RE, analyzing their clinical, electrographic, and neuroimaging features pre-operatively, as well as their postoperative status, including seizure and functional outcomes. All patients with RE who underwent HS in the Epilepsy Surgery Center (CIREP) of the University Hospital of Ribeirão Preto Medical School, between 1995 and 2020 were retrospectively reviewed. Preoperative and postoperative analyses included gender; age at epilepsy onset; seizure semiology; seizure frequency; interictal and ictal electroencephalographic (EEG) findings; age at surgery; duration of epilepsy; surgical complications; duration of follow-up; histopathological findings; and postoperative seizure, cognitive, and functional outcomes. Forty-four patients were evaluated. Mean age at seizure onset and epilepsy duration was 6 years and 2.5 years, respectively. Mean age at surgery was 9 years, with an average follow-up ranging from 3 months to 23 years. All patients presented with severe epilepsy and distinct neurological abnormalities on MRI. Before HS, different degrees of abnormal intellectual performance as well as hemiparesis were seen in 86% and 90%, respectively. Histopathology examination confirmed this diagnosis in 95% patients. At the last follow-up, 68% of patients were seizure free, and 70% were classified as Engel Class I or II. Postoperatively, the cognitive status remained unchanged in 64% of patients. Likewise, the gross motor function remained unchanged in 54% of patients and 74% had functional hand ability after HS. Considering the progressive damage course of RE, hemispheric surgery should be offered to pediatric patients. It has manageable risks and results in good seizure outcome, and the preoperative functional status of these children is often preserved (even when the left hemisphere is involved), thus improving their quality of life.
Unilateral cortical autoimmune encephalitis: A case series and comparison to late-onset Rasmussen's encephalitis.
To report a novel anatomical pattern of autoimmune encephalitis characterized by strictly unilateral cortical inflammation and a clinical picture overlapping with late-onset Rasmussen's encephalitis. We retrospectively gathered data of patients identified at two tertiary referral academic centers who met inclusion criteria. We identified twelve cases (average age 65, +/- 19.8 years, 58% female). All patients had unilateral cortical inflammation manifesting with focal seizures, cognitive decline, hemicortical deficits, and unilateral MRI and/or EEG changes. Six cases were idiopathic, two paraneoplastic, two iatrogenic (in the setting of immune checkpoint inhibitors), and two post-COVID-19. Serologically, ten patients were seronegative, one had high titer anti-GAD65, and one had anti-NMDAR. Five patients met Rasmussen's encephalitis criteria, and six did not fully meet the criteria but had symptoms significantly overlapping with the condition. Most patients had significant improvement with immunotherapy. Unilateral cortical AE seems to be more prevalent in the elderly and more frequently idiopathic and seronegative. Patients with this anatomical variant of autoimmune encephalitis have overlapping features with late-onset Rasmussen's encephalitis but are more responsive to immunotherapy. In cases refractory to immunotherapy, interventions used in refractory Rasmussen's encephalitis may be considered, such as functional hemispherectomy.
Child Neurology: Anti-Hu Encephalitis in an Adolescent With a Mediastinal Seminoma.
Anti-Hu antibodies are associated with autoimmune syndromes, mainly limbic encephalitis, encephalomyelitis, and painful sensory polyneuropathy (Denny-Brown). We report the case of a 15-year-old boy presenting with epilepsia partialis continua (EPC) found to have a right middle frontal gyrus brain lesion without atrophy or contralateral involvement. After partial resection, neuropathology revealed neuronal loss, reactive gliosis and astrocytosis, and perivascular mononuclear inflammatory infiltrate and features of neuronophagia resembling Rasmussen encephalitis. Suboptimal response to antiseizure drugs and surgery prompted further workup with identification of positive serum anti-Hu antibodies and a mediastinal seminoma. The patient was treated with immunotherapy including steroids, IV immunoglobulin, azathioprine, rituximab, plasmapheresis, and mediastinal lesion resection. However, he continued to experience EPC and psychomotor impairment along with left hemiparesis and dysarthria. Given clinical progression with failure to respond to immunotherapy and antiseizure polytherapy, hemispherotomy was attempted and seizure freedom achieved. A review of the literature found only 16 cases of neurologic presentations associated with anti-Hu antibodies in children, confirming the rarity of EPC in these cases. Thus, this report provides a new observation of germ cell mediastinal tumor associated with anti-Hu antibodies in children, broadening the spectrum of anti-Hu-associated neurologic disorders in children and highlighting the importance of considering antineuronal antibody testing in children presenting with EPC and brain lesions suggestive of Rasmussen encephalitis.
Role of Early Intravenous Immunoglobulins in Halting Clinical and Radiographic Disease Progression in Rasmussen Encephalitis.
Rasmussen encephalitis (RE) is a rare progressive presumed autoimmune disorder characterized by pharmacoresistant epilepsy and progressive motor and cognitive deterioration. Despite immunomodulation, more than half of the patients with RE ultimately require functional hemispherotomy. In this study, we evaluated the potential beneficial effects of early initiation of immunomodulation in slowing disease progression and preventing the need for surgical interventions. A retrospective chart review over a 10-year period was conducted at the American University of Beirut Medical Center to identify patients with RE. Data were collected on seizure characteristics, neurological deficits, electroencephalography, brain magnetic resonance imaging results (including volumetric analyses for an objective assessment of radiographic progression), and treatment modalities. Seven patients met the inclusion criteria for RE. All patients received intravenous immunoglobulins (IVIGs) as soon as the diagnosis was entertained. Five patients with only monthly to weekly seizures at the time of IVIG initiation had favorable outcomes without resorting to surgery, along with a relative preservation of the gray matter volumes in the affected cerebral hemispheres. Motor strength was preserved in those patients, and three were seizure free at their last follow-up visit. The two patients who required hemispherotomy were already severely hemiparetic and experiencing daily seizures at the time of IVIG initiation. Our data suggest that the early initiation of IVIG as soon as a diagnosis of RE is suspected, and particularly before the appearance of motor deficits and intractable seizures, can maximize the beneficial effects of immunomodulation in terms of controlling seizures and reducing the rate of cerebral atrophy.
Publicações recentes
The influence of professionals' personal views and values in the development of guidelines for rare diseases: an example from phenylketonuria.
Long-term efficacy and safety of sapropterin in patients who initiated sapropterin at < 4 years of age with phenylketonuria: results of the 3-year extension of the SPARK open-label, multicentre, randomised phase IIIb trial.
🥇 Ensaio randomizadoEmotional and behavioral problems, quality of life and metabolic control in NTBC-treated Tyrosinemia type 1 patients.
Can untreated PKU patients escape from intellectual disability? A systematic review.
🥇 Revisão sistemáticaHighly aggressive pathology of non-functional parathyroid carcinoma.
🥉 Relato de caso📚 EuropePMCmostrando 29
Unilateral cortical autoimmune encephalitis: A case series and comparison to late-onset Rasmussen's encephalitis.
Journal of neuroimmunologyBilateral Rasmussen Encephalitis: Good Outcome Following Hemispherotomy.
Pediatric neurologyThe Important Role of Hemispherotomy for Rasmussen Encephalitis: Clinical and Functional Outcomes.
Pediatric neurologyLong-term seizure outcome and mobility after surgical treatment for Rasmussen encephalitis in children: A single-center experience.
Epileptic disorders : international epilepsy journal with videotapeChild Neurology: Anti-Hu Encephalitis in an Adolescent With a Mediastinal Seminoma.
NeurologyRole of Early Intravenous Immunoglobulins in Halting Clinical and Radiographic Disease Progression in Rasmussen Encephalitis.
Pediatric neurologyTeaching Video NeuroImage: Reflex Seizures Mimicking Paroxysmal Dystonic Movements in a Patient With Late-Onset Rasmussen Encephalitis.
NeurologyEpilepsia partialis continua and unilateral cortical-subcortical FLAIR-hyperintense lesion in Rasmussen's encephalitis: Is it diagnostic?
Epileptic disorders : international epilepsy journal with videotapeEarly Positive Brain 18F-FDG PET and Negative MRI in Rasmussen Encephalitis.
Clinical nuclear medicineCathodal Transcranial Direct Current Stimulation for Treatment of Rasmussen Encephalitis.
NeurologyMolecular and spatial heterogeneity of microglia in Rasmussen encephalitis.
Acta neuropathologica communicationsBrain molecular mechanisms in Rasmussen encephalitis.
EpilepsiaSeizure Outcomes and Reoperation in Surgical Rasmussen Encephalitis Patients.
NeurosurgeryThe Clinical Utility of Surgical Histopathology in Predicting Seizure Outcomes in Patients with Rasmussen Encephalitis Undergoing Hemispherectomy.
World neurosurgeryValproate-Induced Reversible Hemichoreoathetosis in a Patient With Rasmussen Encephalitis.
NeurologyThe influencing factors and changes of cognitive function within 40 Rasmussen encephalitis patients that received a hemispherectomy.
Neurological researchRasmussen encephalitis: Predisposing factors and their potential role in unilaterality.
EpilepsiaBenefits of multi-day supplementation with probiotic kefir in Rasmussen encephalitis: the first case report.
Nutritional neuroscienceUpregulation of adenosine A2A receptor and downregulation of GLT1 is associated with neuronal cell death in Rasmussen's encephalitis.
Brain pathology (Zurich, Switzerland)Motor cortex relocation after complete anatomical hemispherectomy for intractable epilepsy secondary to Rasmussen's encephalitis.
British journal of neurosurgeryNeurons under T Cell Attack Coordinate Phagocyte-Mediated Synaptic Stripping.
CellThe compartmentalized inflammatory response in the multiple sclerosis brain is composed of tissue-resident CD8+ T lymphocytes and B cells.
Brain : a journal of neurologyHumanized mouse model of Rasmussen's encephalitis supports the immune-mediated hypothesis.
The Journal of clinical investigationElevated expression of EBV and TLRs in the brain is associated with Rasmussen's encephalitis.
Virologica SinicaTrapped ipsilateral lateral ventricle: a delayed complication of hemispherotomy for Rasmussen's encephalitis.
BMJ case reportsClinical Applications of Intravenous Immunoglobulins in Child Neurology.
Current pharmaceutical biotechnology[THE ROLE OF AUTOANTIBODIES TO THE EXTRACELLULAR REGIONS OF IONOTROPIC RECEPTORS IN ETIOLOGY AND PATHOGENESIS OF AUTOIMMUNE DISEASES].
Rossiiskii fiziologicheskii zhurnal imeni I.M. SechenovaUpregulation of HMGB1, toll-like receptor and RAGE in human Rasmussen's encephalitis.
Epilepsy researchTranscranial direct current stimulation improves seizure control in patients with Rasmussen encephalitis.
Epileptic disorders : international epilepsy journal with videotapeAssociações
Organizações que acompanham esta doença — pra ter apoio e orientação
Ainda não temos associações cadastradas para Encefalite subaguda de Rasmussen.
É de uma associação que acompanha esta doença? Fale com a gente →
Comunidades
Grupos ativos de quem convive com esta doença aqui no Raras
Ainda não existe comunidade no Raras para Encefalite subaguda de Rasmussen
Pacientes, familiares e cuidadores se organizam em comunidades pra compartilhar experiências, fazer perguntas e se apoiar. Você pode ser o primeiro.
Tire suas dúvidas
Perguntas, dicas e experiências compartilhadas aqui na página
Participe da discussão
Faça login para postar dúvidas, compartilhar experiências e interagir com especialistas.
Fazer loginDoenças relacionadas
Doenças com sintomas parecidos — ajudam quem ainda está buscando diagnóstico
Referências e fontes
Bases de dados externas citadas neste artigo
Publicações científicas
Artigos indexados no PubMed ligados a esta doença no grafo RarasNet — título, periódico e PMID direto da fonte, sem intermediação de IA.
- Bilateral Rasmussen Encephalitis: Good Outcome Following Hemispherotomy.
- The Important Role of Hemispherotomy for Rasmussen Encephalitis: Clinical and Functional Outcomes.
- Unilateral cortical autoimmune encephalitis: A case series and comparison to late-onset Rasmussen's encephalitis.
- Child Neurology: Anti-Hu Encephalitis in an Adolescent With a Mediastinal Seminoma.
- Role of Early Intravenous Immunoglobulins in Halting Clinical and Radiographic Disease Progression in Rasmussen Encephalitis.
- The influence of professionals' personal views and values in the development of guidelines for rare diseases: an example from phenylketonuria.
- Long-term efficacy and safety of sapropterin in patients who initiated sapropterin at < 4 years of age with phenylketonuria: results of the 3-year extension of the SPARK open-label, multicentre, randomised phase IIIb trial.
- Emotional and behavioral problems, quality of life and metabolic control in NTBC-treated Tyrosinemia type 1 patients.
- Can untreated PKU patients escape from intellectual disability? A systematic review.
- Highly aggressive pathology of non-functional parathyroid carcinoma.
Bases de dados e fontes oficiais
Identificadores e referências canônicas usadas para montar este verbete.
- ORPHA:1929(Orphanet)
- MONDO:0016019(MONDO)
- GARD:18752(GARD (NIH))
- Busca completa no PubMed(PubMed)
- Artigo Wikipedia(Wikipedia)
- Q1637701(Wikidata)
Dados compilados pelo RarasNet a partir de fontes abertas (Orphanet, OMIM, MONDO, PubMed/EuropePMC, ClinicalTrials.gov, DATASUS, PCDT/MS). Este conteúdo é informativo e não substitui avaliação médica.
Conteúdo mantido por Agente Raras · Médicos e pesquisadores podem colaborar
Encefalite subaguda de Rasmussen
📋 Origem dos dados
Esta página agrega dados de fontes públicas e oficiais. Dados sobre cobertura no SUS (PCDT, CEAF) são verificados ativamente por agente proativo (ver badge no infobox). Demais dados têm atribuição de fonte + data da última sincronização — clique para abrir o original.
- Doença rara (ontologia)
- fonte: Orphanet
- Identificador unificado
- fonte: MONDO
- Codificação WHO/SUS
- fonte: WHO ICD-10 / DATASUS
- CID-11 (futuro)
- fonte: WHO ICD-11
- NIH/GARD
- fonte: GARD (NIH)
- Indexação biomédica
- fonte: MeSH (NLM)
- Dado público estruturado
- fonte: Wikidata
- Ensaios clínicos
- fonte: ClinicalTrials.gov