A acondroplasia é uma desordem genética cuja principal característica é o nanismo. É a causa mais comum de nanismo e afeta cerca de 1 em cada 27.500 pessoas. Naqueles com a condição, os braços e as pernas são curtos, enquanto o tronco geralmente apresenta um comprimento normal. Os indivíduos afetados têm uma estatura adulta média de 131 centímetros para homens e 123 centímetros para mulheres. Outras características podem incluir uma cabeça aumentada com testa proeminente e subdesenvolvimento da parte central da face. As complicações podem incluir apneia do sono ou infecções de ouvido recorrentes.
Introdução
O que você precisa saber de cara
Visão geral
A Condrodisplasia FGFR3-relacionada é uma doença genética rara que afeta o crescimento dos ossos e cartilagens. A condição é caracterizada por baixa estatura desproporcional, com membros mais curtos em relação ao tronco, e pode envolver alterações na coluna, nas mãos e em outras partes do corpo. A prevalência estimada é de 1 a 9 casos para cada 100.000 pessoas.[1][3]
Sinais e sintomas
Os sinais e sintomas da Condrodisplasia FGFR3-relacionada incluem baixa estatura desproporcional de membros curtos, que pode estar presente desde o nascimento (baixa estatura de membros curtos neonatal). Outros achados frequentes são: retrusão médio-facial (face com aparência de “achatada” no meio), dorso nasal curto, camptodactilia (dedos permanentemente fletidos), encurvamento da fíbula, hipermobilidade da articulação do quadril, cifose lombar na infância e estenose do canal espinhal cervical. Podem ocorrer também dificuldades alimentares, insuficiência respiratória, hipoxemia (baixo oxigênio no sangue) e alterações cardiovasculares. Em alguns casos, há comprometimento cognitivo e cutis laxa palmoplantar (pele frouxa nas palmas e plantas). Sinais como aumento da translucência nucal (detectado em ultrassom pré-natal) e aplasia/hipoplasia dos pulmões ou da mandíbula também foram descritos.[1][3]
Causas genéticas
A Condrodisplasia FGFR3-relacionada é causada por alterações (variantes patogênicas) no gene FGFR3 (Fibroblast Growth Factor Receptor 3). Esse gene fornece instruções para a produção de uma proteína que atua como receptor de fatores de crescimento, essencial para a regulação do crescimento ósseo. Mutações nesse gene levam a um crescimento desordenado da cartilagem e dos ossos.[1][4]
Diagnóstico
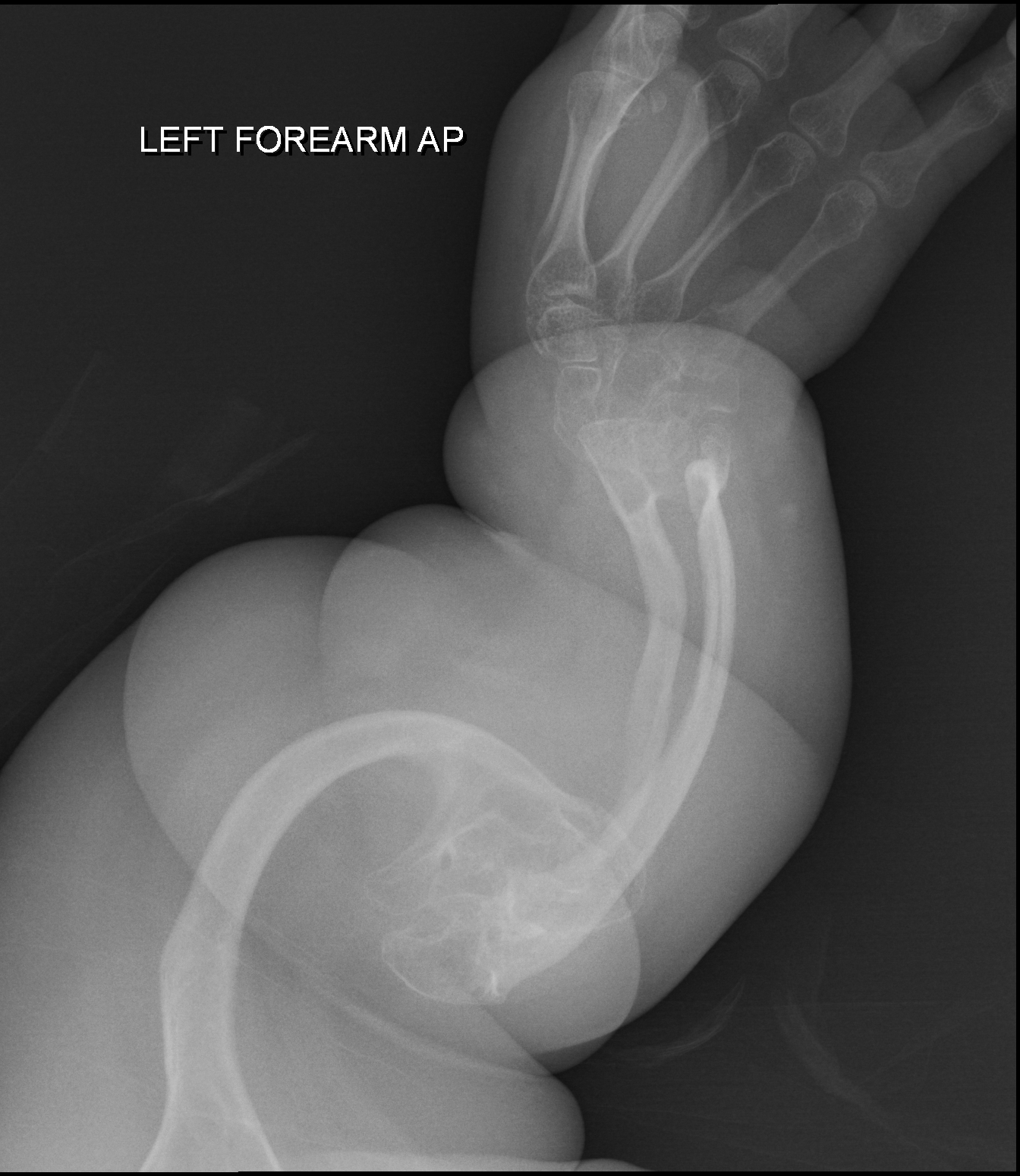
O diagnóstico é baseado na avaliação clínica dos sinais e sintomas característicos, exames de imagem (como radiografias que mostram alterações nos ossos e na coluna) e, principalmente, pela confirmação genética. O teste genético molecular para o gene FGFR3 está disponível (código de teste genético: 336) e existem 416 variantes patogênicas registradas no ClinVar. O diagnóstico diferencial inclui outras condrodisplasias.[1][4]
Tratamento e manejo
O manejo da Condrodisplasia FGFR3-relacionada é multidisciplinar e visa tratar os sintomas e complicações. Pode incluir acompanhamento ortopédico para deformidades ósseas e da coluna, suporte respiratório para insuficiência respiratória, terapia ocupacional e fisioterapia para dificuldades motoras, e suporte nutricional para dificuldades alimentares. O tratamento deve ser individualizado, baseado nas necessidades de cada paciente. Não há medicamentos específicos aprovados para a doença no Brasil, e a condição não possui cobertura pelo SUS para procedimentos específicos.[1]
Prognóstico e qualidade de vida
O prognóstico varia de acordo com a gravidade dos sintomas, especialmente respiratórios e neurológicos. Com acompanhamento adequado e intervenções precoces, muitas pessoas podem ter qualidade de vida significativa, embora a baixa estatura e as limitações físicas possam persistir. O suporte psicológico e a inclusão social são importantes para o bem-estar geral.[1][3]
Conteúdo informativo gerado e mantido automaticamente a partir de fontes oficiais (Orphanet, HPO, OMIM, SUS). Não substitui avaliação médica.
A acondroplasia é uma desordem genética cuja principal característica é o nanismo. É a causa mais comum de nanismo e afeta cerca de 1 em cada 27.500 pessoas. Naqueles com a condição, os braços e as pernas são curtos, enquanto o tronco geralmente apresenta um comprimento normal. Os indivíduos afetados têm uma estatura adulta média de 131 centímetros para homens e 123 centímetros para mulheres. Outras características podem incluir uma cabeça aumentada com testa proeminente e subdesenvolvimento da parte central da face. As complicações podem incluir apneia do sono ou infecções de ouvido recorrentes.
Tem tratamento?
Escala de raridade
<1/50kMuito rara
1/20kRara
1/10kPouco freq.
1/5kIncomum
1/2k
Encontrou um erro ou informação desatualizada? Sugira uma correção →
Entender a doença
Do básico ao detalhe, leia no seu ritmo
Preparando trilha educativa...
Sinais e sintomas
O que aparece no corpo e com que frequência cada sintoma acontece
Visão geral
A Condrodisplasia FGFR3-relacionada é uma doença genética rara que afeta o crescimento dos ossos e cartilagens. A condição é caracterizada por baixa estatura desproporcional, com membros mais curtos em relação ao tronco, e pode envolver alterações na coluna, nas mãos e em outras partes do corpo. A prevalência estimada é de 1 a 9 casos para cada 100.000 pessoas.[1][3]
Sinais e sintomas
Os sinais e sintomas da Condrodisplasia FGFR3-relacionada incluem baixa estatura desproporcional de membros curtos, que pode estar presente desde o nascimento (baixa estatura de membros curtos neonatal). Outros achados frequentes são: retrusão médio-facial (face com aparência de “achatada” no meio), dorso nasal curto, camptodactilia (dedos permanentemente fletidos), encurvamento da fíbula, hipermobilidade da articulação do quadril, cifose lombar na infância e estenose do canal espinhal cervical. Podem ocorrer também dificuldades alimentares, insuficiência respiratória, hipoxemia (baixo oxigênio no sangue) e alterações cardiovasculares. Em alguns casos, há comprometimento cognitivo e cutis laxa palmoplantar (pele frouxa nas palmas e plantas). Sinais como aumento da translucência nucal (detectado em ultrassom pré-natal) e aplasia/hipoplasia dos pulmões ou da mandíbula também foram descritos.[1][3]
Causas genéticas
A Condrodisplasia FGFR3-relacionada é causada por alterações (variantes patogênicas) no gene FGFR3 (Fibroblast Growth Factor Receptor 3). Esse gene fornece instruções para a produção de uma proteína que atua como receptor de fatores de crescimento, essencial para a regulação do crescimento ósseo. Mutações nesse gene levam a um crescimento desordenado da cartilagem e dos ossos.[1][4]
Diagnóstico
O diagnóstico é baseado na avaliação clínica dos sinais e sintomas característicos, exames de imagem (como radiografias que mostram alterações nos ossos e na coluna) e, principalmente, pela confirmação genética. O teste genético molecular para o gene FGFR3 está disponível (código de teste genético: 336) e existem 416 variantes patogênicas registradas no ClinVar. O diagnóstico diferencial inclui outras condrodisplasias.[1][4]
Tratamento e manejo
O manejo da Condrodisplasia FGFR3-relacionada é multidisciplinar e visa tratar os sintomas e complicações. Pode incluir acompanhamento ortopédico para deformidades ósseas e da coluna, suporte respiratório para insuficiência respiratória, terapia ocupacional e fisioterapia para dificuldades motoras, e suporte nutricional para dificuldades alimentares. O tratamento deve ser individualizado, baseado nas necessidades de cada paciente. Não há medicamentos específicos aprovados para a doença no Brasil, e a condição não possui cobertura pelo SUS para procedimentos específicos.[1]
Prognóstico e qualidade de vida
O prognóstico varia de acordo com a gravidade dos sintomas, especialmente respiratórios e neurológicos. Com acompanhamento adequado e intervenções precoces, muitas pessoas podem ter qualidade de vida significativa, embora a baixa estatura e as limitações físicas possam persistir. O suporte psicológico e a inclusão social são importantes para o bem-estar geral.[1][3]
Conteúdo informativo gerado e mantido automaticamente a partir de fontes oficiais (Orphanet, HPO, OMIM, SUS). Não substitui avaliação médica.
Partes do corpo afetadas
+ 68 sintomas em outras categorias
Características mais comuns
Os sintomas variam de pessoa para pessoa. Abaixo estão as 190 características clínicas mais associadas, ordenadas por frequência.
Linha do tempo da pesquisa
Encontrou um erro ou informação desatualizada? Sugira uma correção →
Genética e causas
O que está alterado no DNA e como passa nas famílias
Genes associados
1 gene identificado com associação a esta condição.
Tyrosine-protein kinase that acts as a cell-surface receptor for fibroblast growth factors and plays an essential role in the regulation of cell proliferation, differentiation and apoptosis. Plays an essential role in the regulation of chondrocyte differentiation, proliferation and apoptosis, and is required for normal skeleton development. Regulates both osteogenesis and postnatal bone mineralization by osteoblasts. Promotes apoptosis in chondrocytes, but can also promote cancer cell proliferat
Cell membraneCytoplasmic vesicleEndoplasmic reticulumSecreted
Achondroplasia
A frequent form of short-limb dwarfism. It is characterized by a long, narrow trunk, short extremities, particularly in the proximal (rhizomelic) segments, a large head with frontal bossing, hypoplasia of the midface and a trident configuration of the hands. ACH is an autosomal dominant disease.
Medicamentos e terapias
Mecanismo: Atrial natriuretic peptide receptor B binding agent
Mecanismo: Fibroblast growth factor receptor inhibitor
Mecanismo: Growth hormone receptor agonist
Variantes genéticas (ClinVar)
416 variantes patogênicas registradas no ClinVar.
Classificação de variantes (ClinVar)
Distribuição de 4 variantes classificadas pelo ClinVar.
Vias biológicas (Reactome)
16 vias biológicas associadas aos genes desta condição.
Diagnóstico
Os sinais que médicos procuram e os exames que confirmam
Tratamento e manejo
Remédios, cuidados de apoio e o que precisa acompanhar
Onde tratar no SUS
Hospitais de referência no Brasil e o protocolo oficial do SUS (PCDT)
🇧🇷 Atendimento SUS — Condrodisplasia FGFR3-relacionada
Selecione um estado ou use sua localização para ver resultados.
Dados de DATASUS/CNES, SBGM, ABNeuro e Ministério da Saúde. Sempre confirme a disponibilidade diretamente com o estabelecimento.
Pesquisa ativa
Ensaios clínicos abertos e novidades científicas recentes
Pesquisa e ensaios clínicos
Nenhum ensaio clínico registrado para esta condição.
Publicações mais relevantes
Genetic skeletal disorders: phenotypic-genotypic characteristics and RhGH therapy responses of a pediatric cohort.
This study aimed to explore the genotype-phenotype correlations in individuals with Genetic Skeletal Disorders (GSD), evaluate the efficacy of recombinant human Growth Hormone (rhGH) therapy. The retrospective analysis of the medical records of 80 pediatric patients with GSD diagnosed via whole-exome sequencing was conducted. The therapeutic effects of rhGH treatment were analyzed in 30 of these patients who received rhGH therapy. The study included 80 GSD patients, diagnosed at a median age of 4.88 years, with a median height standard deviation score (Ht-SDS) of - 3.58. The most common clinical manifestations included skeletal deformities (87.5%), short stature (81.3%), and distinctive facial features (including triangular face, abnormality of the philtrum, abnormality of the forehead, etc.) (65.0%). A total of 33 pathogenic genes associated with 20 groups of GSD were identified. The most common groups are Type II collagenopathies (related to the COL2A1 gene) (12/80, 15.0%) and the FGFR3-related chondrodysplasia group (12/80, 15.0%). Those with pathogenic genes linked to Fundamental Cellular Processes had more severe short stature and prenatal phenotypes. Thirty patients received rhGH treatment for a median of 2.25 years (0.33-8.92), showing Ht-SDS increases of 0.66 ± 0.42 and 0.84 ± 0.52, after one and two years, respectively (p < 0.001). Eight untreated patients had an average Ht-SDS decrease of - 0.46 ± 0.55. In this cohort, pediatric GSD patients predominantly presented with short stature, skeletal deformities, and distinctive facial features (including triangular face, abnormality of the philtrum, abnormality of the forehead, etc.), indicating a genotype-phenotype correlation. Compared to untreated GSD patients, those receiving rhGH treatment demonstrated varying degrees of height improvement, however, the long-term efficacy of this treatment warrants further investigation.
Craniofacial growth and function in achondroplasia: a multimodal 3D study on 15 patients.
Achondroplasia is the most frequent FGFR3-related chondrodysplasia, leading to rhizomelic dwarfism, craniofacial anomalies, stenosis of the foramen magnum, and sleep apnea. Craniofacial growth and its correlation with obstructive sleep apnea syndrome has not been assessed in achondroplasia. In this study, we provide a multimodal analysis of craniofacial growth and anatomo-functional correlations between craniofacial features and the severity of obstructive sleep apnea syndrome. A multimodal study was performed based on a paediatric cohort of 15 achondroplasia patients (mean age, 7.8 ± 3.3 years), including clinical and sleep study data, 2D cephalometrics, and 3D geometric morphometry analyses, based on CT-scans (mean age at CT-scan: patients, 4.9 ± 4.9 years; controls, 3.7 ± 4.2 years). Craniofacial phenotype was characterized by maxillo-zygomatic retrusion, deep nasal root, and prominent forehead. 2D cephalometric studies showed constant maxillo-mandibular retrusion, with excessive vertical dimensions of the lower third of the face, and modifications of cranial base angles. All patients with available CT-scan had premature fusion of skull base synchondroses. 3D morphometric analyses showed more severe craniofacial phenotypes associated with increasing patient age, predominantly regarding the midface-with increased maxillary retrusion in older patients-and the skull base-with closure of the spheno-occipital angle. At the mandibular level, both the corpus and ramus showed shape modifications with age, with shortened anteroposterior mandibular length, as well as ramus and condylar region lengths. We report a significant correlation between the severity of maxillo-mandibular retrusion and obstructive sleep apnea syndrome (p < 0.01). Our study shows more severe craniofacial phenotypes at older ages, with increased maxillomandibular retrusion, and demonstrates a significant anatomo-functional correlation between the severity of midface and mandible craniofacial features and obstructive sleep apnea syndrome.
The Effects of Fluvastatin on Indian Hedgehog Pathway in Endochondral Ossification.
Statins have demonstrated to be effective for treating chondrodysplasia and its effects were believed to be associated with the fibroblast growth factor receptor 3 (FGFR3). Statins promoted the degradation of FGFR3 in studies using disease-specific induced pluripotent stem cells and model mice, however, recent studies using normal chondrocytes reported that statins did not degrade FGFR3. In order to further investigate the effects of statins in endochondral ossification, this study examined the influence of statins on Indian hedgehog (Ihh), another important component of endochondral ossification, and its related pathways. The chondrocyte cell line ATDC5 was used to investigate changes in cell proliferation, mRNA, and protein expression levels. In addition, an organ culture of a mouse metatarsal bone was performed followed by hematoxylin-eosin staining and fluorescent immunostaining. Results indicated that expression level of Ihh increased with the addition of statins, which activated the Ihh pathway and altered the localization of Ihh. Changes in cholesterol modification may have affected Ihh diffusibility; however, further experiments are necessary. A reactive increase in parathyroid hormone-related protein (PTHrP) was observed in addition to changes in the Wnt pathway through secreted-related protein 2/3 and low-density lipoprotein 5/6. This led to the promotion of cell proliferation, increase of the hypertrophic chondrocyte layer, inhibition of apoptosis, and decrease in mineralization. This study demonstrated that statins had an influence on Ihh, and that the hyperfunction of Ihh may prevent premature cell death caused by FGFR3-related chondrodysplasia through an indirect increase in the expression of PTHrP.
Statins do not inhibit the FGFR signaling in chondrocytes.
Statins are widely used drugs for cholesterol lowering, which were recently found to counteract the effects of aberrant fibroblast growth factor receptor (FGFR3) signaling in cell and animal models of FGFR3-related chondrodysplasia. This opened an intriguing therapeutic possibility for human dwarfing conditions caused by gain-of-function mutations in FGFR3, although the mechanism of statin action on FGFR3 remains unclear. Here, we determine the effect of statins on FGFR signaling in chondrocytes. Cultured chondrocyte cell lines, mouse embryonic tibia cultures and limb bud micromasses were treated with FGF2 to activate FGFR signaling. The effects of atorvastatin, fluvastatin, lovastatin and pravastatin on FGFR3 protein stability and on FGFR-mediated chondrocyte growth-arrest, loss of extracellular matrix (ECM), induction of premature senescence and hypertrophic differentiation were evaluated. Statins did not alter the level of FGFR3 protein expression nor produce any effect on FGFR-mediated inhibition of chondrocyte proliferation and hypertrophic differentiation in cultured chondrocyte cell lines, mouse tibia cultures or limb bud micromasses. We conclude that statins do not inhibit the FGFR signaling in chondrocytes. Therefore the statin-mediated rescue of FGFR3-related chondrodysplasia, described before, is likely not intrinsic to the growth plate cartilage.
Publicações recentes
Genetic skeletal disorders: phenotypic-genotypic characteristics and RhGH therapy responses of a pediatric cohort.
Craniofacial growth and function in achondroplasia: a multimodal 3D study on 15 patients.
The Effects of Fluvastatin on Indian Hedgehog Pathway in Endochondral Ossification.
Statins do not inhibit the FGFR signaling in chondrocytes.
Children with short-limbed short stature in pediatric endocrinological services in Japan.
📚 EuropePMCmostrando 4
Genetic skeletal disorders: phenotypic-genotypic characteristics and RhGH therapy responses of a pediatric cohort.
Scientific reportsCraniofacial growth and function in achondroplasia: a multimodal 3D study on 15 patients.
Orphanet journal of rare diseasesThe Effects of Fluvastatin on Indian Hedgehog Pathway in Endochondral Ossification.
CartilageStatins do not inhibit the FGFR signaling in chondrocytes.
Osteoarthritis and cartilageAssociações
Organizações que acompanham esta doença — pra ter apoio e orientação
Ainda não temos associações cadastradas para Condrodisplasia FGFR3-relacionada.
É de uma associação que acompanha esta doença? Fale com a gente →
Comunidades
Grupos ativos de quem convive com esta doença aqui no Raras
Ainda não existe comunidade no Raras para Condrodisplasia FGFR3-relacionada
Pacientes, familiares e cuidadores se organizam em comunidades pra compartilhar experiências, fazer perguntas e se apoiar. Você pode ser o primeiro.
Tire suas dúvidas
Perguntas, dicas e experiências compartilhadas aqui na página
Participe da discussão
Faça login para postar dúvidas, compartilhar experiências e interagir com especialistas.
Fazer loginDoenças relacionadas
Doenças com sintomas parecidos — ajudam quem ainda está buscando diagnóstico
Referências e fontes
Bases de dados externas citadas neste artigo
Publicações científicas
Artigos indexados no PubMed ligados a esta doença no grafo RarasNet — título, periódico e PMID direto da fonte, sem intermediação de IA.
- Genetic skeletal disorders: phenotypic-genotypic characteristics and RhGH therapy responses of a pediatric cohort.
- Craniofacial growth and function in achondroplasia: a multimodal 3D study on 15 patients.
- The Effects of Fluvastatin on Indian Hedgehog Pathway in Endochondral Ossification.
- Statins do not inhibit the FGFR signaling in chondrocytes.
- Children with short-limbed short stature in pediatric endocrinological services in Japan.
Bases de dados e fontes oficiais
Identificadores e referências canônicas usadas para montar este verbete.
- ORPHA:93420(Orphanet)
- MONDO:0019685(MONDO)
- GARD:19185(GARD (NIH))
- Variantes catalogadas(ClinVar)
- Busca completa no PubMed(PubMed)
- Q55788796(Wikidata)
Dados compilados pelo RarasNet a partir de fontes abertas (Orphanet, OMIM, MONDO, PubMed/EuropePMC, ClinicalTrials.gov, DATASUS, PCDT/MS). Este conteúdo é informativo e não substitui avaliação médica.
Conteúdo mantido por Agente Raras · Médicos e pesquisadores podem colaborar
Condrodisplasia FGFR3-relacionada
📋 Origem dos dados
Esta página agrega dados de fontes públicas e oficiais. Dados sobre cobertura no SUS (PCDT, CEAF) são verificados ativamente por agente proativo (ver badge no infobox). Demais dados têm atribuição de fonte + data da última sincronização — clique para abrir o original.
- Doença rara (ontologia)
- fonte: Orphanet
- Identificador unificado
- fonte: MONDO
- NIH/GARD
- fonte: GARD (NIH)
- Dado público estruturado
- fonte: Wikidata
- Medicamentos (literatura)
- fonte: Orphanet