Doença metabólica hereditária que tem como base a interrupção do processo metabólico dos carboidratos.
Introdução
O que você precisa saber de cara
Doença metabólica hereditária que tem como base a interrupção do processo metabólico dos carboidratos.
Encontrou um erro ou informação desatualizada? Sugira uma correção →
Entender a doença
Do básico ao detalhe, leia no seu ritmo
Preparando trilha educativa...
Sinais e sintomas
O que aparece no corpo e com que frequência cada sintoma acontece
Partes do corpo afetadas
+ 791 sintomas em outras categorias
Características mais comuns
Os sintomas variam de pessoa para pessoa. Abaixo estão as 1751 características clínicas mais associadas, ordenadas por frequência.
Linha do tempo da pesquisa
Encontrou um erro ou informação desatualizada? Sugira uma correção →
Genética e causas
O que está alterado no DNA e como passa nas famílias
Genes associados
79 genes identificados com associação a esta condição.
Phosphorylase b kinase catalyzes the phosphorylation of serine in certain substrates, including troponin I. The alpha chain may bind calmodulin
Cell membrane
Glycogen storage disease 9A
A metabolic disorder resulting in a mild liver glycogenosis with clinical symptoms that include hepatomegaly, growth retardation, muscle weakness, elevation of glutamate-pyruvate transaminase and glutamate-oxaloacetate transaminase, hypercholesterolemia, hypertriglyceridemia, and fasting hyperketosis. Two subtypes are known: type 1 or classic type with no phosphorylase kinase activity in liver or erythrocytes, and type 2 or variant type with no phosphorylase kinase activity in liver, but normal activity in erythrocytes. Unlike other glycogenosis diseases, glycogen storage disease type 9A is generally a benign condition. Patients improve with age and are often asymptomatic as adults. Accurate diagnosis is therefore also of prognostic interest.
Pyruvate carboxylase catalyzes a 2-step reaction, involving the ATP-dependent carboxylation of the covalently attached biotin in the first step and the transfer of the carboxyl group to pyruvate in the second. Catalyzes in a tissue specific manner, the initial reactions of glucose (liver, kidney) and lipid (adipose tissue, liver, brain) synthesis from pyruvate
Mitochondrion matrix
Pyruvate carboxylase deficiency
Leads to lactic acidosis, intellectual disability and death. It occurs in three forms: mild or type A, severe neonatal or type B, and a very mild lacticacidemia.
Glycogen-branching enzyme participates in the glycogen biosynthetic process along with glycogenin and glycogen synthase. Generates alpha-1,6-glucosidic branches from alpha-1,4-linked glucose chains, to increase solubility of the glycogen polymer (PubMed:26199317, PubMed:8463281, PubMed:8613547)
Glycogen storage disease 4
A metabolic disorder characterized by the accumulation of an amylopectin-like polysaccharide. The typical clinical manifestation is liver disease of childhood, progressing to lethal hepatic cirrhosis. Most children with this condition die before two years of age. However, the liver disease is not always progressive. No treatment apart from liver transplantation has been found to prevent progression of the disease. There is also a neuromuscular form of glycogen storage disease type 4 that varies in onset (perinatal, congenital, juvenile, or adult) and severity.
Catalyzes the removal of sialic acid (N-acetylneuraminic acid) moieties from glycoproteins and glycolipids. To be active, it is strictly dependent on its presence in the multienzyme complex. Appears to have a preference for alpha 2-3 and alpha 2-6 sialyl linkage
Lysosome membraneLysosome lumenCell membraneCytoplasmic vesicleLysosome
Sialidosis
Lysosomal storage disease occurring as two types with various manifestations. Type 1 sialidosis (cherry red spot-myoclonus syndrome or normosomatic type) is late-onset and it is characterized by the formation of cherry red macular spots in childhood, progressive debilitating myoclonus, insiduous visual loss and rarely ataxia. The diagnosis can be confirmed by the screening of the urine for sialyloligosaccharides. Type 2 sialidosis (also known as dysmorphic type) occurs as several variants of increasing severity with earlier age of onset. It is characterized by the presence of abnormal somatic features including coarse facies and dysostosis multiplex, vertebral deformities, intellectual disability, cherry-red spot/myoclonus, sialuria, cytoplasmic vacuolation of peripheral lymphocytes, bone marrow cells and conjunctival epithelial cells.
Removes terminal alpha-N-acetylgalactosamine residues from glycolipids and glycopeptides. Required for the breakdown of glycolipids
Lysosome
Schindler disease
Form of NAGA deficiency characterized by early-onset neuroaxonal dystrophy and neurological signs (convulsion during fever, epilepsy, psychomotor retardation and hypotonia). NAGA deficiency is typically classified in three main phenotypes: NAGA deficiency type I (Schindler disease or Schindler disease type I) with severe manifestations; NAGA deficiency type II (Kanzazi disease or Schindler disease type II) which is mild; NAGA deficiency type III (Schindler disease type III) characterized by mild-to-moderate neurologic manifestations. NAGA deficiency results in the increased urinary excretion of glycopeptides and oligosaccharides containing alpha-N-acetylgalactosaminyl moieties. Inheritance is autosomal recessive.
Serine/threonine-protein kinase which acts as an essential component of the MAP kinase signal transduction pathway. Acts as a MAPK kinase kinase kinase (MAP4K) and is an upstream activator of the stress-activated protein kinase/c-Jun N-terminal kinase (SAP/JNK) signaling pathway and to a lesser extent of the p38 MAPKs signaling pathway. Required for the efficient activation of JNKs by TRAF6-dependent stimuli, including pathogen-associated molecular patterns (PAMPs) such as polyinosine-polycytidi
CytoplasmBasolateral cell membraneGolgi apparatus membrane
Plays an important role in galactose metabolism
Galactosemia 1
A form of galactosemia, an inborn error of galactose metabolism typically manifesting in the neonatal period, after ingestion of galactose, with jaundice, hepatosplenomegaly, hepatocellular insufficiency, food intolerance, hypoglycemia, renal tubular dysfunction, muscle hypotonia, sepsis and cataract. GALAC1 inheritance is autosomal recessive.
Inorganic phosphate and glucose-6-phosphate antiporter of the endoplasmic reticulum. Transports cytoplasmic glucose-6-phosphate into the lumen of the endoplasmic reticulum and translocates inorganic phosphate into the opposite direction (PubMed:33964207). Forms with glucose-6-phosphatase the complex responsible for glucose production through glycogenolysis and gluconeogenesis. Hence, it plays a central role in homeostatic regulation of blood glucose levels
Endoplasmic reticulum membrane
Glycogen storage disease 1B
A metabolic disorder characterized by impairment of terminal steps of glycogenolysis and gluconeogenesis. Patients manifest a wide range of clinical symptoms and biochemical abnormalities, including hypoglycemia, severe hepatomegaly due to excessive accumulation of glycogen, kidney enlargement, growth retardation, lactic acidemia, hyperlipidemia, and hyperuricemia. Glycogen storage disease type 1B patients also present a tendency towards infections associated with neutropenia, relapsing aphthous gingivostomatitis, and inflammatory bowel disease.
Interconverts simultaneously and stereospecifically pyruvate and lactate with concomitant interconversion of NADH and NAD(+)
Cytoplasm
Glycogen storage disease 11
A metabolic disorder that results in exertional myoglobinuria, pain, cramps and easy fatigue.
Multifunctional anion transporter that operates via two distinct transport mechanisms, namely proton-coupled anion cotransport and membrane potential-dependent anion transport (PubMed:15510212, PubMed:21781115, PubMed:22778404, PubMed:23889254). Electroneutral proton-coupled acidic monosaccharide symporter, with a sugar to proton stoichiometry of 1:1. Exports glucuronic acid and free sialic acid derived from sialoglycoconjugate degradation out of lysosomes, driven by outwardly directed lysosomal
Basolateral cell membraneCytoplasmic vesicle, secretory vesicle, synaptic vesicle membraneLysosome membrane
Salla disease
Sialic acid storage disease (SASD). SASDs are autosomal recessive neurodegenerative disorders characterized by hypotonia, cerebellar ataxia and intellectual disability. They are caused by a defect in the metabolism of sialic acid which results in increased urinary excretion of unconjugated sialic acid, specifically N-acetylneuraminic acid. Enlarged lysosomes are seen on electron microscopic studies. Clinical symptoms of SD present usually at age less than 1 year and progression is slow.
Beta-1,3-N-acetylgalactosaminyltransferase that synthesizes a unique carbohydrate structure, GalNAc-beta-1-3GlcNAc, on N- and O-glycans. Has no galactose nor galactosaminyl transferase activity toward any acceptor substrate. Involved in alpha-dystroglycan (DAG1) glycosylation: acts coordinately with GTDC2/POMGnT2 to synthesize a GalNAc-beta3-GlcNAc-beta-terminus at the 4-position of protein O-mannose in the biosynthesis of the phosphorylated O-mannosyl trisaccharide (N-acetylgalactosamine-beta-3
Golgi apparatus membraneEndoplasmic reticulum
Muscular dystrophy-dystroglycanopathy congenital with brain and eye anomalies A11
An autosomal recessive disorder characterized by congenital muscular dystrophy associated with cobblestone lissencephaly and other brain anomalies, eye malformations, profound intellectual disability, and death usually in the first years of life. Included diseases are the more severe Walker-Warburg syndrome and the slightly less severe muscle-eye-brain disease.
Probably involved in connections of major cytoskeletal structures to the plasma membrane. In epithelial cells, required for the formation of microvilli and membrane ruffles on the apical pole. Along with PLEKHG6, required for normal macropinocytosis
Apical cell membraneCell projectionCell projection, microvillus membraneCell projection, ruffle membraneCytoplasm, cell cortexCytoplasm, cytoskeletonCell projection, microvillus
Functions as an activator of NF-kappa-B through increased phosphorylation of the IKK complex. May function in neuronal cells differentiation. May play a role in vesicular transport from endoplasmic reticulum to Golgi
Golgi apparatus, cis-Golgi networkEndoplasmic reticulumCytoplasm
Intellectual developmental disorder, autosomal recessive 13
A disorder characterized by significantly below average general intellectual functioning associated with impairments in adaptive behavior and manifested during the developmental period. Brain magnetic resonance imaging of MRT13 patients indicates the presence of mild cerebral white matter hypoplasia. Microcephaly is present in some but not all affected individuals.
Component of the nuclear pore complex (NPC), a complex required for the trafficking across the nuclear envelope. Functions as a scaffolding element in the nuclear phase of the NPC essential for normal nucleocytoplasmic transport of proteins and mRNAs, plays a role in the establishment of nuclear-peripheral chromatin compartmentalization in interphase, and in the mitotic spindle checkpoint signaling during mitosis. Involved in the quality control and retention of unspliced mRNAs in the nucleus; i
NucleusNucleus membraneNucleus envelopeNucleus, nuclear pore complexCytoplasmCytoplasm, cytoskeleton, spindleChromosome, centromere, kinetochore
Catalyzes the methylation of 5-carboxymethyl uridine to 5-methylcarboxymethyl uridine at the wobble position of the anticodon loop in tRNA via its methyltransferase domain (PubMed:20123966, PubMed:20308323, PubMed:31079898). Catalyzes the last step in the formation of 5-methylcarboxymethyl uridine at the wobble position of the anticodon loop in target tRNA (PubMed:20123966, PubMed:20308323). Has a preference for tRNA(Arg) and tRNA(Glu), and does not bind tRNA(Lys) (PubMed:20308323). Binds tRNA a
CytoplasmNucleus
Intellectual developmental disorder, autosomal recessive 71
A form of intellectual disability, a disorder characterized by significantly below average general intellectual functioning associated with impairments in adaptive behavior and manifested during the developmental period. MRT71 features include impaired intellectual development, global developmental delay, mildly delayed walking, poor language, seizures in the first years of life, and behavioral abnormalities.
Component of the FERRY complex (Five-subunit Endosomal Rab5 and RNA/ribosome intermediary) (PubMed:37267905). The FERRY complex directly interacts with mRNAs and RAB5A, and functions as a RAB5A effector involved in the localization and the distribution of specific mRNAs most likely by mediating their endosomal transport. The complex recruits mRNAs and ribosomes to early endosomes through direct mRNA-interaction (PubMed:37267905). Plays a role in mast cell degranulation
CytoplasmEarly endosome
Intellectual developmental disorder, autosomal recessive 66
A disorder characterized by significantly below average general intellectual functioning associated with impairments in adaptive behavior and manifested during the developmental period. MRT66 patients have intellectual disability, delayed speech development, neuropsychiatric symptoms, and relatively normal life span.
Required for ciliogenesis and for structural integrity at the ciliary tip
Cell projection, ciliumCytoplasm, cytoskeleton, microtubule organizing center, centrosome, centrioleCytoplasm, cytoskeleton, microtubule organizing center, centrosomeCytoplasm, cytoskeleton, spindle pole
Joubert syndrome 25
A form of Joubert syndrome, a disorder presenting with cerebellar ataxia, oculomotor apraxia, hypotonia, neonatal breathing abnormalities and psychomotor delay. Neuroradiologically, it is characterized by cerebellar vermian hypoplasia/aplasia, thickened and reoriented superior cerebellar peduncles, and an abnormally large interpeduncular fossa, giving the appearance of a molar tooth on transaxial slices (molar tooth sign). Additional variable features include retinal dystrophy, renal disease, liver fibrosis, and polydactyly. JBTS25 clinical manifestations appear to be confined to the neurologic system. JBTS25 inheritance is autosomal recessive.
Acyltransferase which catalyzes the transfer of an acyl group from an acyl-CoA to a lysophosphatidylinositol (1-acylglycerophosphatidylinositol or LPI) leading to the production of a phosphatidylinositol (1,2-diacyl-sn-glycero-3-phosphoinositol or PI) and participates in the reacylation step of the phospholipid remodeling pathway also known as the Lands cycle (PubMed:18094042, PubMed:18772128). Prefers arachidonoyl-CoA as the acyl donor, thus contributing to the regulation of free levels arachid
Endoplasmic reticulum membrane
Intellectual developmental disorder, autosomal recessive 57
A disorder characterized by significantly below average general intellectual functioning associated with impairments in adaptive behavior and manifested during the developmental period. MRT57 patients have moderate to severe intellectual disability, and delayed psychomotor development with poor or absent speech. Some patients manifest seizures and autistic features.
E3 ubiquitin-protein ligase component of the LUBAC complex which conjugates linear ('Met-1'-linked) polyubiquitin chains to substrates and plays a key role in NF-kappa-B activation and regulation of inflammation (PubMed:17006537, PubMed:19136968, PubMed:20005846, PubMed:21455173, PubMed:21455180, PubMed:21455181, PubMed:22863777, PubMed:28189684, PubMed:28481331). LUBAC conjugates linear polyubiquitin to IKBKG and RIPK1 and is involved in activation of the canonical NF-kappa-B and the JNK signal
Cytoplasm
Immunodeficiency 115 with autoinflammation
An autosomal recessive immunologic disorder manifesting in early infancy and characterized by combined immunodeficiency, recurrent bacterial, viral, and fungal infections, as well as autoinflammatory features, including arthritis and dermatitis.
Hydrolyzes 6-sulfate groups in N-acetyl-d-glucosaminide units of heparin sulfate and keratan sulfate
Lysosome
Mucopolysaccharidosis 3D
A form of mucopolysaccharidosis type 3, an autosomal recessive lysosomal storage disease due to impaired degradation of heparan sulfate. MPS3 is characterized by severe central nervous system degeneration, but only mild somatic disease. Onset of clinical features usually occurs between 2 and 6 years; severe neurologic degeneration occurs in most patients between 6 and 10 years of age, and death occurs typically during the second or third decade of life.
Together with PDHA1 forms the heterotetrameric E1 subunit of the pyruvate dehydrogenase (PDH) complex (PubMed:17474719, PubMed:19081061). The PDH complex catalyzes the overall conversion of pyruvate to acetyl-CoA and CO(2), and thereby links cytoplasmic glycolysis and the mitochondrial tricarboxylic acid (TCA) cycle (Probable). It contains multiple copies of three enzymatic components: pyruvate dehydrogenase (E1), dihydrolipoamide acetyltransferase (E2) and dihydrolipoamide dehydrogenase (E3) (P
Mitochondrion matrix
Pyruvate dehydrogenase E1-beta deficiency
An enzymatic defect causing primary lactic acidosis in children. It is associated with a broad clinical spectrum ranging from fatal lactic acidosis in the newborn to chronic neurologic dysfunction with structural abnormalities in the central nervous system without systemic acidosis.
Enzyme with hydroxy-pyruvate reductase, glyoxylate reductase and D-glycerate dehydrogenase enzymatic activities. Reduces hydroxypyruvate to D-glycerate, glyoxylate to glycolate, oxidizes D-glycerate to hydroxypyruvate
Hyperoxaluria primary 2
A disorder characterized by elevated urinary excretion of oxalate and L-glycerate, progressive tissue accumulation of insoluble calcium oxalate, nephrolithiasis, nephrocalcinosis, and end-stage renal disease.
Catalyzes the transfer of a phosphate from ATP to alpha-D-galactose and participates in the first committed step in the catabolism of galactose
Galactosemia 2
A form of galactosemia, an inborn error of galactose metabolism typically manifesting in the neonatal period, after ingestion of galactose, with jaundice, hepatosplenomegaly, hepatocellular insufficiency, food intolerance, hypoglycemia, renal tubular dysfunction, muscle hypotonia, sepsis and cataract. GALAC2 inheritance is autosomal recessive.
Magnesium-independent polyisoprenoid diphosphatase that catalyzes the sequential dephosphorylation of presqualene, farnesyl, geranyl and geranylgeranyl diphosphates (PubMed:16464866, PubMed:19220020, PubMed:20110354). Functions in the innate immune response through the dephosphorylation of presqualene diphosphate which acts as a potent inhibitor of the signaling pathways contributing to polymorphonuclear neutrophils activation (PubMed:16464866, PubMed:23568778). May regulate the biosynthesis of
Endoplasmic reticulum membraneNucleus envelopeNucleus inner membrane
The pyruvate dehydrogenase (PDH) complex, catalyzes the overall conversion of pyruvate to acetyl-CoA and CO(2), and thereby links cytoplasmic glycolysis and the mitochondrial tricarboxylic acid (TCA) cycle (Probable). It contains multiple copies of three enzymatic components: pyruvate dehydrogenase (E1), dihydrolipoamide acetyltransferase (E2) and dihydrolipoamide dehydrogenase (E3); (Probable). Within this complex, the catalytic function of this enzyme is to accept, and to transfer to coenzyme
Mitochondrion matrix
Catalyzes a step in lysosomal heparan sulfate degradation
Lysosome
Mucopolysaccharidosis 3A
A severe form of mucopolysaccharidosis type 3, an autosomal recessive lysosomal storage disease due to impaired degradation of heparan sulfate. MPS3 is characterized by severe central nervous system degeneration, but only mild somatic disease. Onset of clinical features usually occurs between 2 and 6 years; severe neurologic degeneration occurs in most patients between 6 and 10 years of age, and death occurs typically during the second or third decade of life. MPS3A is characterized by earlier onset, rapid progression of symptoms and shorter survival.
Non-catalytic component of the RNA exosome complex which has 3'->5' exoribonuclease activity and participates in a multitude of cellular RNA processing and degradation events. In the nucleus, the RNA exosome complex is involved in proper maturation of stable RNA species such as rRNA, snRNA and snoRNA, in the elimination of RNA processing by-products and non-coding 'pervasive' transcripts, such as antisense RNA species and promoter-upstream transcripts (PROMPTs), and of mRNAs with processing defe
CytoplasmNucleusNucleus, nucleolusNucleus, nucleoplasm
Pontocerebellar hypoplasia 1D
An autosomal recessive neurologic disorder with onset at birth or in infancy, and characterized by progressive axonal motor neuronopathy, severe generalized hypotonia, respiratory insufficiency, and cerebellar atrophy. Death in childhood may occur.
Serine/threonine kinase involved in the regulation of key cellular processes including the cell cycle, nuclear condensation, transcription regulation, and DNA damage response (PubMed:14645249, PubMed:18617507, PubMed:19103756, PubMed:33076429). Controls chromatin organization and remodeling by mediating phosphorylation of histone H3 on 'Thr-4' and histone H2AX (H2aXT4ph) (PubMed:31527692, PubMed:37179361). It also phosphorylates KAT5 in response to DNA damage, promoting KAT5 association with chr
NucleusCytoplasmNucleus, Cajal body
Pontocerebellar hypoplasia 1A
A form of pontocerebellar hypoplasia, a disorder characterized by structural defects of the pons and cerebellum, evident upon brain imaging. PCH1A is an autosomal recessive form characterized by an abnormally small cerebellum and brainstem, central and peripheral motor dysfunction from birth, gliosis and spinal cord anterior horn cells degeneration resembling infantile spinal muscular atrophy. Additional features include muscle hypotonia, congenital contractures and respiratory insufficiency that is evident at birth.
Non-catalytic component of the RNA exosome complex which has 3'->5' exoribonuclease activity and participates in a multitude of cellular RNA processing and degradation events. In the nucleus, the RNA exosome complex is involved in proper maturation of stable RNA species such as rRNA, snRNA and snoRNA, in the elimination of RNA processing by-products and non-coding 'pervasive' transcripts, such as antisense RNA species and promoter-upstream transcripts (PROMPTs), and of mRNAs with processing defe
CytoplasmNucleusNucleus, nucleolus
Pontocerebellar hypoplasia 1C
A severe autosomal recessive neurodegenerative disease characterized by cerebellar and corpus callosum hypoplasia, abnormal myelination of the central nervous system, and spinal motor neuron disease. Affected individuals manifest failure to thrive, severe muscle weakness, spasticity and psychomotor retardation. Vision and hearing are impaired.
Regulator subunit of pancreatic ATP-sensitive potassium channel (KATP), playing a major role in the regulation of insulin release. In pancreatic cells, it forms KATP channels with KCNJ11; KCNJ11 forms the channel pore while ABCC8 is required for activation and regulation
Cell membrane
Leucine-induced hypoglycemia
Rare cause of hypoglycemia and is described as a condition in which symptomatic hypoglycemia is provoked by high protein feedings. Hypoglycemia is also elicited by administration of oral or intravenous infusions of a single amino acid, leucine.
Lysosomal enzyme involved in the degradation pathway of dermatan sulfate and heparan sulfate
Lysosome
Mucopolysaccharidosis 2
An X-linked lysosomal storage disease characterized by intracellular accumulation of heparan sulfate and dermatan sulfate and their excretion in urine. Most children with MPS2 have a severe form with early somatic abnormalities including skeletal deformities, hepatosplenomegaly, and progressive cardiopulmonary deterioration. A prominent feature is neurological damage that presents as developmental delay and hyperactivity but progresses to intellectual disability and dementia. They die before 15 years of age, usually as a result of obstructive airway disease or cardiac failure. In contrast, those with a mild form of MPS2 may survive into adulthood, with attenuated somatic complications and often without intellectual disability.
Required for anchoring dihydrolipoamide dehydrogenase (E3) to the dihydrolipoamide transacetylase (E2) core of the pyruvate dehydrogenase complexes of eukaryotes. This specific binding is essential for a functional PDH complex
Mitochondrion matrix
Pyruvate dehydrogenase E3-binding protein deficiency
A metabolic disorder characterized by decreased activity of the pyruvate dehydrogenase complex without observable reduction in the activities of enzymes E1, E2, or E3. Clinical features include hypotonia and psychomotor retardation.
Has a role in alternative splicing and transcription regulation (PubMed:29522154). Involved in both constitutive and alternative pre-mRNA splicing. May have a role in the recognition of the 3' splice site during the second step of splicing
NucleusNucleus speckleCytoplasm
Intellectual developmental disorder, autosomal recessive 70
A form of intellectual disability, a disorder characterized by significantly below average general intellectual functioning associated with impairments in adaptive behavior and manifested during the developmental period. MRT70 patients manifest impaired intellectual development, mild facial dysmorphism, febrile seizures, and behavioral abnormalities.
Mitochondrial fatty acid beta-oxidation enzyme that catalyzes the third step of the beta-oxidation cycle for medium and short-chain 3-hydroxy fatty acyl-CoAs (C4 to C10) (PubMed:10231530, PubMed:11489939, PubMed:16725361). Plays a role in the control of insulin secretion by inhibiting the activation of glutamate dehydrogenase 1 (GLUD1), an enzyme that has an important role in regulating amino acid-induced insulin secretion (By similarity). Plays a role in the maintenance of normal spermatogenesi
Mitochondrion matrix
3-alpha-hydroxyacyl-CoA dehydrogenase deficiency
An autosomal recessive, metabolic disorder with various clinical presentations including hypoglycemia, hepatoencephalopathy, myopathy or cardiomyopathy, and in some cases sudden death.
Triosephosphate isomerase is an extremely efficient metabolic enzyme that catalyzes the interconversion between dihydroxyacetone phosphate (DHAP) and D-glyceraldehyde-3-phosphate (G3P) in glycolysis and gluconeogenesis It is also responsible for the non-negligible production of methylglyoxal a reactive cytotoxic side-product that modifies and can alter proteins, DNA and lipids
Cytoplasm
Triosephosphate isomerase deficiency
An autosomal recessive multisystem disorder characterized by congenital hemolytic anemia, progressive neuromuscular dysfunction, susceptibility to bacterial infection, and cardiomyopathy.
Hydrolyzes glucose-6-phosphate to glucose in the endoplasmic reticulum. Forms with the glucose-6-phosphate transporter (SLC37A4/G6PT) the complex responsible for glucose production in the terminal step of glycogenolysis and gluconeogenesis. Hence, it is the key enzyme in homeostatic regulation of blood glucose levels
Endoplasmic reticulum membrane
Glycogen storage disease 1A
A metabolic disorder characterized by impairment of terminal steps of glycogenolysis and gluconeogenesis. Patients manifest a wide range of clinical symptoms and biochemical abnormalities, including hypoglycemia, severe hepatomegaly due to excessive accumulation of glycogen, kidney enlargement, growth retardation, lactic acidemia, hyperlipidemia, and hyperuricemia.
Lipoamide dehydrogenase is a component of the glycine cleavage system as well as an E3 component of three alpha-ketoacid dehydrogenase complexes (pyruvate-, alpha-ketoglutarate-, and branched-chain amino acid-dehydrogenase complex) (PubMed:15712224, PubMed:16442803, PubMed:16770810, PubMed:17404228, PubMed:20160912, PubMed:20385101). The 2-oxoglutarate dehydrogenase complex is mainly active in the mitochondrion (PubMed:29211711). A fraction of the 2-oxoglutarate dehydrogenase complex also locali
Mitochondrion matrixNucleusCell projection, cilium, flagellumCytoplasmic vesicle, secretory vesicle, acrosome
Dihydrolipoamide dehydrogenase deficiency
An autosomal recessive metabolic disorder characterized biochemically by a combined deficiency of the branched-chain alpha-keto acid dehydrogenase complex (BCKDC), pyruvate dehydrogenase complex (PDC), and alpha-ketoglutarate dehydrogenase complex (KGDC). Clinically, affected individuals have lactic acidosis and neurologic deterioration due to sensitivity of the central nervous system to defects in oxidative metabolism.
Together with PDHB forms the heterotetrameric E1 subunit of the pyruvate dehydrogenase (PDH) complex (PubMed:17474719, PubMed:19081061). The PDH complex catalyzes the overall conversion of pyruvate to acetyl-CoA and CO(2), and thereby links cytoplasmic glycolysis and the mitochondrial tricarboxylic acid (TCA) cycle (PubMed:19081061, PubMed:7782287). It contains multiple copies of three enzymatic components: pyruvate dehydrogenase (E1), dihydrolipoamide acetyltransferase (E2) and dihydrolipoamide
Mitochondrion matrix
Pyruvate dehydrogenase E1-alpha deficiency
An enzymatic defect causing primary lactic acidosis in children. It is associated with a broad clinical spectrum ranging from fatal lactic acidosis in the newborn to chronic neurologic dysfunction with structural abnormalities in the central nervous system without systemic acidosis.
Non-catalytic component of the RNA exosome complex which has 3'->5' exoribonuclease activity and participates in a multitude of cellular RNA processing and degradation events. In the nucleus, the RNA exosome complex is involved in proper maturation of stable RNA species such as rRNA, snRNA and snoRNA, in the elimination of RNA processing by-products and non-coding 'pervasive' transcripts, such as antisense RNA species and promoter-upstream transcripts (PROMPTs), and of mRNAs with processing defe
CytoplasmNucleus, nucleolusNucleus
Pontocerebellar hypoplasia 1B
A severe autosomal recessive neurologic disorder characterized by a combination of cerebellar and spinal motor neuron degeneration beginning at birth. There is diffuse muscle weakness, progressive microcephaly, global developmental delay, and brainstem involvement.
E3 ubiquitin-protein ligase, which accepts ubiquitin from specific E2 ubiquitin-conjugating enzymes, such as UBE2L3/UBCM4, and then transfers it to substrates (PubMed:12629548, PubMed:17449468, PubMed:18711448). Functions as an E3 ligase for oxidized IREB2 and both heme and oxygen are necessary for IREB2 ubiquitination (PubMed:12629548). Promotes ubiquitination of TAB2 and IRF3 and their degradation by the proteasome (PubMed:17449468, PubMed:18711448). Component of the LUBAC complex which conjug
Polyglucosan body myopathy 1 with or without immunodeficiency
A disease characterized by polyglucosan storage myopathy associated with early-onset progressive muscle weakness and progressive dilated cardiomyopathy, which may necessitate cardiac transplant in severe cases. Some patients present with severe immunodeficiency, invasive bacterial infections and chronic autoinflammation.
Lysosome
Mucopolysaccharidosis 1H
A severe form of mucopolysaccharidosis type 1, a rare lysosomal storage disease characterized by progressive physical deterioration with urinary excretion of dermatan sulfate and heparan sulfate. Patients with MPS1H usually present, within the first year of life, a combination of hepatosplenomegaly, skeletal deformities, corneal clouding and severe intellectual disability. Obstructive airways disease, respiratory infection and cardiac complications usually result in death before 10 years of age.
Non-receptor tyrosine kinase involved in B-lymphocyte development, differentiation and signaling (By similarity). B-cell receptor (BCR) signaling requires a tight regulation of several protein tyrosine kinases and phosphatases, and associated coreceptors (By similarity). Binding of antigen to the B-cell antigen receptor (BCR) triggers signaling that ultimately leads to B-cell activation (By similarity). Signaling through BLK plays an important role in transmitting signals through surface immunog
Cell membrane
Maturity-onset diabetes of the young 11
A form of diabetes that is characterized by an autosomal dominant mode of inheritance, onset in childhood or early adulthood (usually before 25 years of age), a primary defect in insulin secretion and frequent insulin-independence at the beginning of the disease.
Insulin decreases blood glucose concentration. It increases cell permeability to monosaccharides, amino acids and fatty acids. It accelerates glycolysis, the pentose phosphate cycle, and glycogen synthesis in liver
Secreted
Hyperproinsulinemia
An autosomal dominant condition characterized by elevated levels of serum proinsulin-like material.
CytoplasmCytoplasm, cytoskeleton
Acts as accessory component of the N-oligosaccharyl transferase (OST) complex which catalyzes the transfer of a high mannose oligosaccharide from a lipid-linked oligosaccharide donor to an asparagine residue within an Asn-X-Ser/Thr consensus motif in nascent polypeptide chains. Involved in N-glycosylation of STT3B-dependent substrates. Specifically required for the glycosylation of a subset of acceptor sites that are near cysteine residues; in this function seems to act redundantly with MAGT1. I
Endoplasmic reticulum membrane
Intellectual developmental disorder, autosomal recessive 7
A disorder characterized by significantly below average general intellectual functioning associated with impairments in adaptive behavior and manifested during the developmental period.
Actin-binding protein that is involved in actin cytoskeleton assembly and reorganization (PubMed:21730168, PubMed:22330775). Acts as an actin nucleation factor and promotes assembly of actin filaments together with SPIRE1 and SPIRE2 (PubMed:21730168, PubMed:22330775). Involved in intracellular vesicle transport along actin fibers, providing a novel link between actin cytoskeleton dynamics and intracellular transport (By similarity). Required for asymmetric spindle positioning, asymmetric oocyte
Cytoplasm, cytoskeletonCytoplasm, cytosolCytoplasm, perinuclear regionNucleusNucleus, nucleolusCell membraneCytoplasmic vesicle membraneCytoplasm, cell cortex
Intellectual developmental disorder, autosomal recessive 47
A disorder characterized by significantly below average general intellectual functioning associated with impairments in adaptive behavior and manifested during the developmental period. MRT47 patients show delayed development, with cognition and speech more affected than motor skills.
Histone methyltransferase that dimethylates histone H3 at 'Arg-17', forming asymmetric dimethylarginine (H3R17me2a), leading to activate transcription via chromatin remodeling (By similarity). Maternal factor involved in epigenetic chromatin reprogramming of the paternal genome in the zygote: mediates H3R17me2a, promoting histone H3.3 incorporation in the male pronucleus, leading to TET3 recruitment and subsequent DNA demethylation (By similarity)
NucleusCytoplasm
Intellectual developmental disorder, autosomal recessive 44
A disorder characterized by significantly below average general intellectual functioning associated with impairments in adaptive behavior and manifested during the developmental period. MRT44 manifestations include mild to severe cognitive impairment, delayed psychomotor development, seizures in some patients, and dysmorphic features.
Acts as a component of the WASH core complex that functions as a nucleation-promoting factor (NPF) at the surface of endosomes, where it recruits and activates the Arp2/3 complex to induce actin polymerization, playing a key role in the fission of tubules that serve as transport intermediates during endosome sorting
Early endosome
Intellectual developmental disorder, autosomal recessive 43
A disorder characterized by significantly below average general intellectual functioning associated with impairments in adaptive behavior and manifested during the developmental period.
Adapter protein that associates with PIDD1 and the caspase CASP2 to form the PIDDosome, a complex that activates CASP2 and triggers apoptosis (PubMed:15073321, PubMed:16652156, PubMed:17159900, PubMed:17289572, PubMed:9044836). Also recruits CASP2 to the TNFR-1 signaling complex through its interaction with RIPK1 and TRADD and may play a role in the tumor necrosis factor-mediated signaling pathway (PubMed:8985253)
CytoplasmNucleus
Intellectual developmental disorder, autosomal recessive 34, with variant lissencephaly
A disorder characterized by mild to moderate intellectual disability, megalencephaly or enlarged head circumference, and a mild variant of lissencephaly with anterior-predominant pachygyria with shallow and unusually wide sulci and mildly thickened cortex. Some patients may have seizures.
Mutarotase that catalyzes the interconversion of beta-D-galactose and alpha-D-galactose during galactose metabolism (PubMed:12753898). Beta-D-galactose is metabolized in the liver into glucose 1-phosphate, the primary metabolic fuel, by the action of four enzymes that constitute the Leloir pathway: GALM, GALK1 (galactokinase), GALT (galactose-1-phosphate uridylyltransferase) and GALE (UDP-galactose-4'-epimerase) (PubMed:30451973). Involved in the maintenance of the equilibrium between the beta-
Cytoplasm
Galactosemia 4
A form of galactosemia, an inborn error of galactose metabolism typically manifesting in the neonatal period, after ingestion of galactose, with jaundice, hepatosplenomegaly, hepatocellular insufficiency, food intolerance, hypoglycemia, renal tubular dysfunction, muscle hypotonia, sepsis and cataract. GALAC4 inheritance is autosomal recessive.
Facilitative glucose transporter, which is responsible for constitutive or basal glucose uptake (PubMed:10227690, PubMed:10954735, PubMed:18245775, PubMed:19449892, PubMed:25982116, PubMed:27078104, PubMed:32860739). Has a very broad substrate specificity; can transport a wide range of aldoses including both pentoses and hexoses (PubMed:18245775, PubMed:19449892). Most important energy carrier of the brain: present at the blood-brain barrier and assures the energy-independent, facilitative trans
Cell membraneMelanosomePhotoreceptor inner segment
GLUT1 deficiency syndrome 1
A neurologic disorder showing wide phenotypic variability. The most severe 'classic' phenotype comprises infantile-onset epileptic encephalopathy associated with delayed development, acquired microcephaly, motor incoordination, and spasticity. Onset of seizures, usually characterized by apneic episodes, staring spells, and episodic eye movements, occurs within the first 4 months of life. Other paroxysmal findings include intermittent ataxia, confusion, lethargy, sleep disturbance, and headache. Varying degrees of cognitive impairment can occur, ranging from learning disabilities to severe intellectual disability.
Interconverts simultaneously and stereospecifically pyruvate and lactate with concomitant interconversion of NADH and NAD(+)
CytoplasmMitochondrion inner membrane
Lactate dehydrogenase B deficiency
A condition with no deleterious effects on health. LDHBD is of interest to laboratory medicine mainly because it can cause misdiagnosis in those disorders in which elevation of serum LDH is expected.
Electrogenic Na(+)-coupled sugar symporter that actively transports D-glucose at the plasma membrane, with a Na(+) to sugar coupling ratio of 1:1 (PubMed:20980548, PubMed:28592437, PubMed:34880493, PubMed:37217492, PubMed:38057552). Transporter activity is driven by a transmembrane Na(+) electrochemical gradient set by the Na(+)/K(+) pump (PubMed:20980548, PubMed:28592437, PubMed:34880493). Unlike SLC5A1/SGLT1, requires the auxiliary protein PDZK1IP1/MAP17 for full transporter activity (PubMed:3
Apical cell membrane
Renal glucosuria
A disorder characterized by persistent isolated glucosuria, normal fasting serum glucose concentration, decreased renal tubular resorption of glucose from the urine, and absence of any other signs of tubular dysfunction.
Essential for the degradation of glycogen in lysosomes (PubMed:14695532, PubMed:18429042, PubMed:1856189, PubMed:7717400). Has highest activity on alpha-1,4-linked glycosidic linkages, but can also hydrolyze alpha-1,6-linked glucans (PubMed:29061980)
LysosomeLysosome membrane
Pompe disease, infantile-onset
An early-onset form of Pompe disease, an autosomal recessive lysosomal storage disease characterized by lysosomal alpha-glucosidase deficiency, a broad clinical spectrum and age at onset ranging from infancy to adulthood. The classic early-onset form of IOPD presents at birth with massive accumulation of glycogen in muscle, heart and liver. Cardiomyopathy and muscular hypotonia are the cardinal features of this form whose life expectancy is less than two years. A milder infantile form manifests as progressive muscular disorder of childhood and patients have better prognosis.
E3 ubiquitin-protein ligase. Together with the phosphatase EPM2A/laforin, appears to be involved in the clearance of toxic polyglucosan and protein aggregates via multiple pathways. In complex with EPM2A/laforin and HSP70, suppresses the cellular toxicity of misfolded proteins by promoting their degradation through the ubiquitin-proteasome system (UPS). Ubiquitinates the glycogen-targeting protein phosphatase subunits PPP1R3C/PTG and PPP1R3D in a laforin-dependent manner and targets them for pro
Endoplasmic reticulumNucleus
Myoclonic epilepsy of Lafora 2
A form of progressive myoclonic epilepsy, a clinically and genetically heterogeneous group of disorders defined by the combination of action and reflex myoclonus, other types of epileptic seizures, and progressive neurodegeneration and neurocognitive impairment. MELF2 is an autosomal recessive, severe form characterized by onset of progressive neurodegeneration between 8 and 18 years of age. Initial features can include headache, myoclonic jerks, generalized seizures, and often visual hallucination. Typically, as seizures increase in frequency, cognitive function declines towards dementia, and affected individuals die usually within 10 years after onset. At the cellular level, MELF2 is characterized by accumulation of starch-like polyglucosans called Lafora bodies (LBs) that are most abundant in organs with the highest glucose metabolism: brain, heart, liver and skeletal muscle.
Removes sulfate groups from chondroitin-4-sulfate (C4S) and regulates its degradation (PubMed:19306108). Involved in the regulation of cell adhesion, cell migration and invasion in colonic epithelium (PubMed:19306108). In the central nervous system, is a regulator of neurite outgrowth and neuronal plasticity, acting through the control of sulfate glycosaminoglycans and neurocan levels (By similarity)
LysosomeCell surface
Mucopolysaccharidosis 6
A form of mucopolysaccharidosis, a group of lysosomal storage diseases characterized by defective degradation of glycosaminoglycans, resulting in their excessive accumulation and secretion. The diseases are progressive and often display a wide spectrum of clinical severity. MPS6 is an autosomal recessive form characterized by intracellular accumulation of dermatan sulfate. Clinical features can include abnormal growth, short stature, stiff joints, skeletal malformations, corneal clouding, hepatosplenomegaly, and cardiac abnormalities.
Catalyzes the hydrolysis of a wide range of substrates including cholesteryl esters, phospholipids, lysophospholipids, di- and tri-acylglycerols, and fatty acid esters of hydroxy fatty acids (FAHFAs) (PubMed:10220579, PubMed:27509211, PubMed:27650499, PubMed:8471055). Preferentially hydrolyzes FAHFAs with the ester bond further away from the carboxylate. Unsaturated FAHFAs are hydrolyzed more quickly than saturated FAHFAs (By similarity). Has an essential role in the complete digestion of dietar
Secreted
Maturity-onset diabetes of the young 8 with exocrine dysfunction
An autosomal dominant form of diabetes characterized by a primary defect in insulin secretion, exocrine pancreatic dysfunction, altered pancreatic morphology, recurrent abdominal pain, and fecal elastase deficiency. Disease onset is at less than 25 years of age.
Transcription factor (PubMed:10207080, PubMed:9748269). Activates the epsilon- and gamma-globin gene promoters and, to a much lower degree, the beta-globin gene and represses promoters containing SP1-like binding inhibiting cell growth (PubMed:10207080, PubMed:16131492, PubMed:9748269). Represses transcription of SMAD7 which enhances TGF-beta signaling (By similarity). Induces apoptosis (By similarity)
Nucleus
Maturity-onset diabetes of the young 7
A form of diabetes that is characterized by an autosomal dominant mode of inheritance, onset in childhood or early adulthood (usually before 25 years of age), a primary defect in insulin secretion and frequent insulin-independence at the beginning of the disease.
Plays an important role in the differentiation and development of pancreatic islet beta cells. Transcriptional repressor that binds to a common element in the glucagon, insulin and somatostatin promoters. Competes with PAX6 for this same promoter binding site. Isoform 2 appears to be a dominant negative form antagonizing PAX4 transcriptional activity
Nucleus
Type 2 diabetes mellitus
A multifactorial disorder of glucose homeostasis caused by a lack of sensitivity to insulin. Affected individuals usually have an obese body habitus and manifestations of a metabolic syndrome characterized by diabetes, insulin resistance, hypertension and hypertriglyceridemia. The disease results in long-term complications that affect the eyes, kidneys, nerves, and blood vessels.
Transcriptional regulator which controls the expression of hepatic genes during the transition of endodermal cells to hepatic progenitor cells, facilitating the recruitment of RNA pol II to the promoters of target genes (PubMed:30597922). Activates the transcription of CYP2C38 (By similarity). Represses the CLOCK-BMAL1 transcriptional activity and is essential for circadian rhythm maintenance and period regulation in the liver and colon cells (PubMed:30530698)
Nucleus
Maturity-onset diabetes of the young 1
A form of diabetes that is characterized by an autosomal dominant mode of inheritance, onset in childhood or early adulthood (usually before 25 years of age), a primary defect in insulin secretion and frequent insulin-independence at the beginning of the disease.
Involved in the Hedgehog (Hh) signaling pathway, is essential for normal ciliogenesis (PubMed:29263200). Regulates the proteolytic processing of GLI3 and cooperates with the transcription factor EMX1 in the induction of downstream Hh pathway gene expression and gonadotropin-releasing hormone production (PubMed:29263200). WDR11 complex facilitates the tethering of Adaptor protein-1 complex (AP-1)-derived vesicles. WDR11 complex acts together with TBC1D23 to facilitate the golgin-mediated capture
Cytoplasm, cytoskeleton, cilium basal bodyCytoplasmNucleusCytoplasm, cytoskeleton, cilium axonemeCytoplasmic vesicleGolgi apparatus, trans-Golgi network
Component of the eukaryotic translation initiation factor 3 (eIF-3) complex, which is required for several steps in the initiation of protein synthesis (PubMed:17581632, PubMed:25849773, PubMed:27462815). The eIF-3 complex associates with the 40S ribosome and facilitates the recruitment of eIF-1, eIF-1A, eIF-2:GTP:methionyl-tRNAi and eIF-5 to form the 43S pre-initiation complex (43S PIC). The eIF-3 complex stimulates mRNA recruitment to the 43S PIC and scanning of the mRNA for AUG recognition. T
Cytoplasm
Intellectual developmental disorder, autosomal recessive 67
A form of intellectual disability, a disorder characterized by significantly below average general intellectual functioning associated with impairments in adaptive behavior and manifested during the developmental period. Some MRT67 patients manifest seizures and sensorineural hearing loss.
Histone demethylase that demethylates 'Lys-4' of histone H3, thereby playing a central role in histone code (PubMed:24952722, PubMed:27214403, PubMed:28262558). Does not demethylate histone H3 'Lys-9' or H3 'Lys-27'. Demethylates trimethylated, dimethylated and monomethylated H3 'Lys-4'. Acts as a transcriptional corepressor for FOXG1B and PAX9. Favors the proliferation of breast cancer cells by repressing tumor suppressor genes such as BRCA1 and HOXA5 (PubMed:24952722). In contrast, may act as
Nucleus
Intellectual developmental disorder, autosomal recessive 65
A disorder characterized by significantly below average general intellectual functioning associated with impairments in adaptive behavior and manifested during the developmental period. MRT65 patients have moderate to severe intellectual disability, developmental delay, and facial dysmorphism. Camptodactyly is present in some patients.
Required for transcriptional activation subsequent to the assembly of the pre-initiation complex (By similarity). Component of the Mediator complex, a coactivator involved in the regulated transcription of nearly all RNA polymerase II-dependent genes. Mediator functions as a bridge to convey information from gene-specific regulatory proteins to the basal RNA polymerase II transcription machinery. Mediator is recruited to promoters by direct interactions with regulatory proteins and serves as a s
Nucleus
Intellectual developmental disorder, autosomal recessive 18, with or without epilepsy
A disorder characterized by significantly below average general intellectual functioning associated with impairments in adaptive behavior and manifested during the developmental period.
Intestinal trehalase is probably involved in the hydrolysis of ingested trehalose
Cell membrane
Trehalase deficiency
An autosomal recessive condition characterized by the inability to digest trehalose, a disaccharide found in mushrooms, products containing baker's yeast, and dried food. Individuals with trehalase deficiency suffer from abdominal pain, increased rectal flatulence, and diarrhea due to osmotic water flow into the colon.
Catalyzes the rate-limiting step of the non-oxidative phase in the pentose phosphate pathway. Catalyzes the reversible conversion of sedheptulose-7-phosphate and D-glyceraldehyde 3-phosphate into erythrose-4-phosphate and beta-D-fructose 6-phosphate (PubMed:18687684, PubMed:8955144). Not only acts as a pentose phosphate pathway enzyme, but also affects other metabolite pathways by altering its subcellular localization between the nucleus and the cytoplasm (By similarity)
NucleusCytoplasm
Transaldolase deficiency
An inborn error of the pentose phosphate pathway resulting in early-onset multisystem disease. Clinical features include growth retardation, dysmorphic features, cutis laxa, congenital heart disease, hepatosplenomegaly, telangiectases of the skin, pancytopenia, and bleeding tendency.
Catalyzes the reversible conversion of ribose-5-phosphate to ribulose 5-phosphate and participates in the first step of the non-oxidative branch of the pentose phosphate pathway
Ribose 5-phosphate isomerase deficiency
An autosomal recessive inborn error of polyols metabolism characterized by highly elevated level of ribitol and arabitol in brain and body fluids. Clinical features include leukoencephalopathy, psychomotor retardation from early life, neurologic regression, and a mild sensorimotor neuropathy.
Nucleus
Phosphorylase b kinase catalyzes the phosphorylation of serine in certain substrates, including troponin I. The alpha chain may bind calmodulin
Cell membrane
Glycogen storage disease 9D
A metabolic disorder characterized by slowly progressive, predominantly distal muscle weakness and atrophy. Clinical features include exercise intolerance with early fatigability, pain, cramps and occasionally myoglobinuria.
Lysosomal acetyltransferase that acetylates the non-reducing terminal alpha-glucosamine residue of intralysosomal heparin or heparan sulfate, converting it into a substrate for luminal alpha-N-acetyl glucosaminidase
Lysosome membrane
Mucopolysaccharidosis 3C
A form of mucopolysaccharidosis type 3, an autosomal recessive lysosomal storage disease due to impaired degradation of heparan sulfate. MPS3 is characterized by severe central nervous system degeneration, but only mild somatic disease. Onset of clinical features usually occurs between 2 and 6 years; severe neurologic degeneration occurs in most patients between 6 and 10 years of age, and death occurs typically during the second or third decade of life.
Plays an important role in the degradation of dermatan and keratan sulfates
Lysosome
Mucopolysaccharidosis 7
A form of mucopolysaccharidosis, a group of lysosomal storage diseases characterized by defective degradation of glycosaminoglycans, resulting in their excessive accumulation and secretion. The diseases are progressive and often display a wide spectrum of clinical severity. MPS7 is an autosomal recessive form with a highly variable phenotype, ranging from severe lethal hydrops fetalis to mild forms with survival into adulthood. Most patients with the intermediate phenotype show hepatomegaly, skeletal anomalies, coarse facies, and variable degrees of mental impairment.
Inward rectifier potassium channel that forms the pore of ATP-sensitive potassium channels (KATP), regulating potassium permeability as a function of cytoplasmic ATP and ADP concentrations in many different cells (PubMed:29286281, PubMed:34815345). Inward rectifier potassium channels are characterized by a greater tendency to allow potassium to flow into the cell rather than out of it. Their voltage dependence is regulated by the concentration of extracellular potassium; as external potassium is
Membrane
Hyperinsulinemic hypoglycemia, familial, 2
A form of hyperinsulinemic hypoglycemia, a clinically and genetically heterogeneous disorder characterized by inappropriate insulin secretion from the pancreatic beta-cells in the presence of low blood glucose levels. HHF2 is a common cause of persistent hypoglycemia in infancy. Unless early and aggressive intervention is undertaken, brain damage from recurrent episodes of hypoglycemia may occur. HHF2 inheritance can be autosomal dominant or autosomal recessive.
Activates insulin, somatostatin, glucokinase, islet amyloid polypeptide and glucose transporter type 2 gene transcription. Particularly involved in glucose-dependent regulation of insulin gene transcription. As part of a PDX1:PBX1b:MEIS2b complex in pancreatic acinar cells is involved in the transcriptional activation of the ELA1 enhancer; the complex binds to the enhancer B element and cooperates with the transcription factor 1 complex (PTF1) bound to the enhancer A element. Binds preferentiall
NucleusCytoplasm, cytosol
Pancreatic agenesis 1
A disease characterized by isolated hypoplasia or agenesis of the pancreas, pancreatic beta-cell failure resulting in neonatal insulin-dependent diabetes mellitus, and exocrine pancreatic insufficiency.
ATPase involved both in DNA repair and rescue of stalled ribosomes (PubMed:22055184, PubMed:28757607, PubMed:32099016, PubMed:32579943, PubMed:36302773). 3'-5' DNA helicase involved in repair of alkylated DNA: promotes DNA unwinding to generate single-stranded substrate needed for ALKBH3, enabling ALKBH3 to process alkylated N3-methylcytosine (3mC) within double-stranded regions (PubMed:22055184). Also involved in activation of the ribosome quality control (RQC) pathway, a pathway that degrades
NucleusNucleus speckleCytoplasm, cytosol
Intellectual developmental disorder, autosomal recessive 81
An autosomal recessive disorder characterized by variable features including mild to severe developmental delay, hypotonia, feeding difficulties, extreme fatigue, and neurobehavioral abnormalities.
Associates with the adapter-like complex 4 (AP-4) and may therefore play a role in vesicular trafficking of proteins at the trans-Golgi network
Cytoplasm, cytosolCell membrane
Intellectual developmental disorder, autosomal recessive 61
A disorder characterized by significantly below average general intellectual functioning associated with impairments in adaptive behavior and manifested during the developmental period. MRT61 patients manifest delayed psychomotor development, moderate to severe intellectual disability, and variable dysmorphic facial features. Refractory seizures and brain abnormalities are present in severely affected patients.
Ionotropic glutamate receptor that functions as a cation-permeable ligand-gated ion channel, gated by L-glutamate and the glutamatergic agonist kainic acid (PubMed:7536611, PubMed:8730589, PubMed:14511640). L-glutamate acts as an excitatory neurotransmitter at many synapses in the central nervous system (By similarity). Binding of the excitatory neurotransmitter L-glutamate induces a conformational change leading to the opening of the cation channel, converting the chemical signal to an electric
Cell membranePostsynaptic cell membrane
Intellectual developmental disorder, autosomal recessive 6
A disorder characterized by significantly below average general intellectual functioning associated with impairments in adaptive behavior and manifested during the developmental period. MRT6 patients display mild to severe intellectual disability and psychomotor development delay in early childhood. Patients do not have neurologic problems, congenital malformations, or facial dysmorphism. Body height, weight, and head circumference are normal.
Phosphatase involved in the dephosphorylation of myo-inositol monophosphates to generate myo-inositol (PubMed:17068342, PubMed:8718889, PubMed:9462881). Is also able to dephosphorylate scyllo-inositol-phosphate, myo-inositol 1,4-diphosphate, scyllo-inositol-1,3-diphosphate and scyllo-inositol-1,4-diphosphate (PubMed:17068342). Also dephosphorylates in vitro other sugar-phosphates including D-galactose-1-phosphate, glucose-1-phosphate, glucose-6-phosphate, fructose-1-phosphate, beta-glycerophosph
Cytoplasm
Intellectual developmental disorder, autosomal recessive 59
A disorder characterized by significantly below average general intellectual functioning associated with impairments in adaptive behavior and manifested during the developmental period.
Adenosine kinase that mediates the phosphorylation of the purine nucleoside adenosine at the 5' position in an ATP-dependent manner: catalyzes phosphorylation of both unmodified and modified adenosines (PubMed:21963049, PubMed:40840445, PubMed:6246102, PubMed:8577746, PubMed:9070863). Plays a key role in the detoxification of modified adenosines containing N(6)-methylated adenine (m6A) post-transcriptional modification (PubMed:40840445). Modified nucleosides are derived from the degradation of R
Cytoplasm, cytosolNucleusCytoplasm
Hypermethioninemia due to adenosine kinase deficiency
A metabolic disorder characterized by global developmental delay, early-onset seizures, mild dysmorphic features, and characteristic biochemical anomalies, including persistent hypermethioninemia with increased levels of S-adenosylmethionine and S-adenosylhomocysteine. Homocysteine levels are typically normal.
Mitochondrial carbonic anhydrase that catalyzes the reversible conversion of carbon dioxide to bicarbonate/HCO3 (PubMed:24530203, PubMed:8356065). Mitochondria are impermeable to HCO3, and thus this intramitochondrial carbonic anhydrase is pivotal in providing HCO3 for multiple mitochondrial enzymes that catalyze the formation of essential metabolites of intermediary metabolism in the urea and Krebs cycles (PubMed:24530203)
Mitochondrion
Hyperammonemia due to carbonic anhydrase VA deficiency
An autosomal recessive inborn error of metabolism, clinically characterized by infantile hyperammonemic encephalopathy. Metabolic abnormalities include hypoglycemia, hyperlactatemia, metabolic acidosis and respiratory alkalosis.
Variantes genéticas (ClinVar)
947 variantes patogênicas registradas no ClinVar.
Vias biológicas (Reactome)
186 vias biológicas associadas aos genes desta condição.
Diagnóstico
Os sinais que médicos procuram e os exames que confirmam
Tratamento e manejo
Remédios, cuidados de apoio e o que precisa acompanhar
Onde tratar no SUS
Hospitais de referência no Brasil e o protocolo oficial do SUS (PCDT)
🇧🇷 Atendimento SUS — Doença do metabolismo dos carboidratos
Centros de Referência SUS
21 centros habilitados pelo SUS para Doença do metabolismo dos carboidratos
Centros para Doença do metabolismo dos carboidratos
Detalhes dos centros
Hospital Universitário Prof. Edgard Santos (HUPES)
R. Dr. Augusto Viana, s/n - Canela, Salvador - BA, 40110-060 · CNES 0003808
Serviço de Referência
Hospital de Apoio de Brasília (HAB)
AENW 3 Lote A Setor Noroeste - Plano Piloto, Brasília - DF, 70684-831 · CNES 0010456
Serviço de Referência
Hospital Estadual Infantil e Maternidade Alzir Bernardino Alves (HIABA)
Av. Min. Salgado Filho, 918 - Soteco, Vila Velha - ES, 29106-010 · CNES 6631207
Serviço de Referência
Hospital das Clínicas da UFG
Rua 235 QD. 68 Lote Área, Nº 285, s/nº - Setor Leste Universitário, Goiânia - GO, 74605-050 · CNES 2338424
Serviço de Referência
Hospital das Clínicas da UFMG
Av. Prof. Alfredo Balena, 110 - Santa Efigênia, Belo Horizonte - MG, 30130-100 · CNES 2280167
Serviço de Referência
NUPAD / Faculdade de Medicina UFMG
Av. Prof. Alfredo Balena, 189 - 5 andar - Centro, Belo Horizonte - MG, 30130-100 · CNES 2183226
Serviço de Referência
Hospital Universitário João de Barros Barreto
R. dos Mundurucus, 4487 - Guamá, Belém - PA, 66073-000 · CNES 2337878
Serviço de Referência
Hospital de Clínicas da Universidade Federal de Pernambuco
Av. Prof. Moraes Rego, 1235 - Cidade Universitária, Recife - PE, 50670-901 · CNES 2561492
Atenção Especializada
Instituto de Medicina Integral Prof. Fernando Figueira (IMIP)
R. dos Coelhos, 300 - Boa Vista, Recife - PE, 50070-902 · CNES 0000647
Serviço de Referência
Hospital de Clínicas da UFPR
R. Gen. Carneiro, 181 - Alto da Glória, Curitiba - PR, 80060-900 · CNES 2364980
Serviço de Referência
Hospital Universitário Pedro Ernesto (HUPE-UERJ)
Blvd. 28 de Setembro, 77 - Vila Isabel, Rio de Janeiro - RJ, 20551-030 · CNES 2280221
Serviço de Referência
Instituto Nacional de Saúde da Mulher, da Criança e do Adolescente Fernandes Figueira (IFF/Fiocruz)
Av. Rui Barbosa, 716 - Flamengo, Rio de Janeiro - RJ, 22250-020 · CNES 2269988
Serviço de Referência
Hospital Universitário Onofre Lopes (HUOL)
Av. Nilo Peçanha, 620 - Petrópolis, Natal - RN, 59012-300 · CNES 2408570
Atenção Especializada
Hospital São Lucas da PUCRS
Av. Ipiranga, 6690 - Jardim Botânico, Porto Alegre - RS, 90610-000 · CNES 2232928
Serviço de Referência
Hospital de Clínicas de Porto Alegre (HCPA)
Rua Ramiro Barcelos, 2350 Bloco A - Av. Protásio Alves, 211 - Bloco B e C - Santa Cecília, Porto Alegre - RS, 90035-903 · CNES 2237601
Serviço de Referência
Hospital Universitário da UFSC (HU-UFSC)
R. Profa. Maria Flora Pausewang - Trindade, Florianópolis - SC, 88036-800 · CNES 2560356
Serviço de Referência
Hospital das Clínicas da FMUSP
R. Dr. Ovídio Pires de Campos, 225 - Cerqueira César, São Paulo - SP, 05403-010 · CNES 2077485
Serviço de Referência
Hospital de Clínicas da UNICAMP
R. Vital Brasil, 251 - Cidade Universitária, Campinas - SP, 13083-888 · CNES 2748223
Serviço de Referência
Hospital de Clínicas de Ribeirão Preto (HCRP-USP)
R. Ten. Catão Roxo, 3900 - Vila Monte Alegre, Ribeirão Preto - SP, 14015-010 · CNES 2082187
Serviço de Referência
Instituto da Criança e do Adolescente (ICr-HCFMUSP)
Av. Dr. Enéas Carvalho de Aguiar, 647 - Cerqueira César, São Paulo - SP, 05403-000 · CNES 2081695
Serviço de Referência
UNIFESP / Hospital São Paulo
R. Napoleão de Barros, 715 - Vila Clementino, São Paulo - SP, 04024-002 · CNES 2688689
Serviço de Referência
Dados de DATASUS/CNES, SBGM, ABNeuro e Ministério da Saúde. Sempre confirme a disponibilidade diretamente com o estabelecimento.
Pesquisa ativa
Ensaios clínicos abertos e novidades científicas recentes
Ensaios em destaque
🟢 Recrutando agora
1 pesquisa recrutando participantes. Converse com seu médico sobre a possibilidade de participar.
Outros ensaios clínicos
5 ensaios clínicos encontrados, 1 ativos.
Publicações mais relevantes
Untargeted Proteomics Profiling of Liver and Plasma in Fed and Fasted Liver-Specific Glycogen Storage Disease Type Ia (GSD Ia) Mice: Toward Potential Protein Biomarkers.
Glycogen storage disease type Ia (GSD Ia) is a rare autosomal recessive inherited disorder of carbohydrate metabolism, caused by a deficiency in glucose 6-phosphatase-α (G6PC1). Patients primarily suffer from failure to thrive, hepatomegaly, and severe fasting intolerance, biochemically characterized by hypoketotic, hypoglycemia, and hyperlipidemia. Because of clinical and biochemical heterogeneity, identifying biomarkers is imperative for prognosis and monitoring. An untargeted proteomics workflow was employed for identifying protein changes in liver and plasma from hepatocyte-specific G6pc knockout mice under fed and fasted conditions. This links the effect of hepatic G6Pase/G6pc deficiency to circulating protein biomarkers and allows assessment of the relationship with different clinical circumstances and long-term complications. In the liver, the main differences between hepatic GSD Ia mice versus controls were observed in proteins related to carbohydrate and lipid metabolism, proteasome, ribosome, NAD+ metabolism, and mitochondria. In GSD Ia mouse plasma, proteins were mainly down-regulated in the complement and coagulation cascades. Effects in hepatic GSD Ia mice were in general more pronounced under fasting conditions. Several potential biomarkers that showed significant alterations in both liver and plasma were identified. These include proteins involved in carbohydrate and lipid metabolism (e.g., UGP2, ALDOB, and FASN), complement and coagulation cascades (SERPINA1E, C8b, and MBL2), 20S proteasome subunits (PSMA4, PSMA7, and PSMB5), and the electron transport chain (SDHA). Their consistent changes observed in both the liver and circulation indicate their potential as circulating biomarkers reflecting liver condition. Together with their reported associations with liver diseases, we hypothesize that they could monitor hepatic complications.
A 2-year-old girl with merged phenotypes: galactosemia and Coffin-Lowry syndrome.
Galactosemia is a congenital disorder of carbohydrate metabolism, in which the body is unable to metabolize galactose properly. Coffin-Lowry syndrome (CLS) is characterized by intellectual disability, developmental delay, dysmorphic features, growth retardation, vision and hearing loss, and skeletal changes, which is an X-linked disorder, with males being more severely affected, whereas the clinical findings in females show variability. This case is presented due to the rare concomitance of galactosemia and CLS. A 2-year-old female patient, previously diagnosed with galactosemia, who had good dietary adherence was noticed to have developmental delay, dysmorphic features, nephrolithiasis and recurrent pericardial effusions during follow-up. Further research was carried out to diagnose an underlying second disease. Metabolic tests were inconclusive. Clinical exome sequencing (CES) analysis, revealed a heterozygous c.472C>T p. (Arg158Cys) pathogenic variant in RPS6KA3 (OMIM #300075) and CLS (OMIM #303600) was diagnosed. This case report is a unique summary of a patient with galactosemia who further was diagnosed with CLS that emphasizes the possibility of co-occurrence of rare diseases and highlights the importance of conducting further investigations in patients with unexplained findings in the context of existing metabolic diseases.
Neuromuscular pathology and mitochondrial dysfunction in sorbitol dehydrogenase gene-related distal hereditary motor neuropathies.
Biallelic variants in sorbitol dehydrogenase (SORD) have been reported to be a major cause of autosomal recessive distal hereditary motor neuropathy (dHMN). In this study, the clinical and pathological features of 10 patients with SORD gene-related dHMN are reported. Homozygous c.757delG variant was detected in 6 patients while c.757delG, c.786 + 1G>A, c.218C>T, and a novel c.104T>A compound heterozygous variants were observed in the others. Serum sorbitol, xylitol, and D-arabinitol were measured by gas chromatography-mass spectrometry; increased sorbitol and xylitol, and decreased D-arabinitol were identified. Sural nerve biopsies showed mild loss of large, myelinated fibers, and a few thin myelinated fibers. Skeletal muscle biopsies exhibited a neurogenic pattern with vacuoles, tubular aggregates, and abnormal mitochondria. Proteomic analyses of muscle tissue were performed to explore potential mechanisms. Complex I deficiency was dominant in the proteomic analysis and the malic acid/oxaloacetic acid ratio was significantly higher in the patients than in controls. In summary, SORD gene-related dHMN is a systemic disorder of carbohydrate metabolism with subclinical myopathologic changes, including tubular aggregates and vacuoles. Mitochondrial complex I deficiency, may be a key mechanism in SORD gene-related dHMN.
A machine learning model accurately identifies glycogen storage disease Ia patients based on plasma acylcarnitine profiles.
Glycogen storage disease (GSD) Ia is an ultra-rare inherited disorder of carbohydrate metabolism. Patients often present in the first months of life with fasting hypoketotic hypoglycemia and hepatomegaly. The diagnosis of GSD Ia relies on a combination of different biomarkers, mostly routine clinical chemical markers and subsequent genetic confirmation. However, a specific and reliable biomarker is lacking. As GSD Ia patients demonstrate altered lipid metabolism and mitochondrial fatty acid oxidation, we built a machine learning model to identify GSD Ia patients based on plasma acylcarnitine profiles. We collected plasma acylcarnitine profiles from 3958 patients, of whom 31 have GSD Ia. Synthetic samples were generated to address the problem of class imbalance in the dataset. We built several machine learning models based on gradient-boosted trees. Our approach included hyperparameter tuning and feature selection and generalization was checked using both nested cross-validation and a held-out test set. The binary classifier was able to correctly identify 5/6 GSD Ia patients in a held-out test set without generating significant amounts of false positive results. The best model showed excellent performance with a mean received operator curve (ROC) AUC of 0.955 and precision-recall (PR) curve AUC of 0.674 in nested CV. This study demonstrates an innovative approach to applying machine learning to ultra-rare diseases by accurately identifying GSD Ia patients based on plasma free carnitine and acylcarnitine concentrations, leveraging subtle acylcarnitine abnormalities. Acylcarnitine features that were strong predictors for GSD Ia include C16-carnitine, C14OH-carnitine, total carnitine and acetylcarnitine. The model demonstrated high sensitivity and specificity, with selected parameters that were not only robust but also highly interpretable. Our approach offers potential prospect for the inclusion of GSD Ia in newborn screening. Rare diseases are underrepresented in machine learning studies and this work highlights the potential for these techniques, even in ultra-rare diseases such as GSD Ia.
Multiomics approach provides insight into altered choline metabolism and liver injury in patients with glycogen storage disease type Ia.
Glycogen storage disease type Ia (GSDIa) is an inherited disorder of carbohydrate metabolism. Patients present with excessive storage of glycogen and fat in the liver and kidneys and are potentially at risk of developing long-term complications. Currently, the mainstay of treatment is highly tailored dietary regimens aimed at improving metabolic control. In the present study, to better elucidate the mechanisms potentially involved in the development of long-term complications, a mass spectrometry-based strategy was employed for an in-depth characterization of the serum proteomic and metabolomic profile of n.12 GSDIa patients. The detection of differential abundance of highly liver-specific circulating proteins and choline-related metabolites in patients provides new insights into the extent of liver damage and dysregulation of lipid metabolism in GSDIa. Specifically, the differential abundance of serum aldolase B and its positive correlation with traditional liver function markers supports its role as a potential biomarker for long-term monitoring of GSDIa liver injury.
Publicações recentes
Untargeted Proteomics Profiling of Liver and Plasma in Fed and Fasted Liver-Specific Glycogen Storage Disease Type Ia (GSD Ia) Mice: Toward Potential Protein Biomarkers.
A 2-year-old girl with merged phenotypes: galactosemia and Coffin-Lowry syndrome.
Multiomics approach provides insight into altered choline metabolism and liver injury in patients with glycogen storage disease type Ia.
Neuromuscular pathology and mitochondrial dysfunction in sorbitol dehydrogenase gene-related distal hereditary motor neuropathies.
A machine learning model accurately identifies glycogen storage disease Ia patients based on plasma acylcarnitine profiles.
📚 EuropePMC16 artigos no totalmostrando 42
Untargeted Proteomics Profiling of Liver and Plasma in Fed and Fasted Liver-Specific Glycogen Storage Disease Type Ia (GSD Ia) Mice: Toward Potential Protein Biomarkers.
Journal of inherited metabolic diseaseA 2-year-old girl with merged phenotypes: galactosemia and Coffin-Lowry syndrome.
Journal of pediatric endocrinology & metabolism : JPEMMultiomics approach provides insight into altered choline metabolism and liver injury in patients with glycogen storage disease type Ia.
Scientific reportsNeuromuscular pathology and mitochondrial dysfunction in sorbitol dehydrogenase gene-related distal hereditary motor neuropathies.
Journal of neuropathology and experimental neurologyA machine learning model accurately identifies glycogen storage disease Ia patients based on plasma acylcarnitine profiles.
Orphanet journal of rare diseasesFactors affecting the quality of life in pregnant women with diabetes: the mediating effect of illnesses acceptance.
BMC pregnancy and childbirthFanconi-Bickel syndrome complicated by nephrocalcinosis and GFR decline.
Pediatric nephrology (Berlin, Germany)Classic Galactosemia: Clinical and Computational Characterization of a Novel GALT Missense Variant (p.A303D) and a Literature Review.
International journal of molecular sciencesEffects of microcystin on protein profile in hepatopancreas of Litopenaeus vannamei.
Ying yong sheng tai xue bao = The journal of applied ecologyCaregivers' nutrition-related knowledge, perceptions, practices and barriers regarding the therapeutic diet for classical galactosaemia.
Journal of human nutrition and dietetics : the official journal of the British Dietetic AssociationAddition of galactose-1-phosphate measurement enhances newborn screening for classical galactosemia.
Journal of inherited metabolic diseaseUnderstanding the Role of GLUT2 in Dysglycemia Associated with Fanconi-Bickel Syndrome.
BiomedicinesThe progress of pluripotent stem cell-derived pancreatic β-cells regeneration for diabetic therapy.
Frontiers in endocrinologyDiagnostic Code-Based Screening for Identifying Children with Primary Hyperoxaluria.
The Journal of urologyGalactosemia: Biochemistry, Molecular Genetics, Newborn Screening, and Treatment.
BiomoleculesUnderstanding the Mechanism of Dysglycemia in a Fanconi-Bickel Syndrome Patient.
Frontiers in endocrinologyUnderstanding the role of SGLT2 inhibitors in glycogen storage disease type Ib: the experience of one UK centre.
Orphanet journal of rare diseasesPediatric metanephric adenoma with Fanconi-Bickel syndrome: a case report and review of literature.
Surgical case reportsAssociation between fetal vascular malperfusion and gestational diabetes.
The journal of obstetrics and gynaecology researchModifiable factors affecting renal preservation in type I glycogen storage disease after liver transplantation: a single-center propensity-match cohort study.
Orphanet journal of rare diseasesAbnormal N-glycan fucosylation, galactosylation, and sialylation of IgG in adults with classical galactosemia, influence of dietary galactose intake.
JIMD reportsAssessment of α-amylase and α-glucosidase inhibitory potential of Citrus reticulata peel extracts in hyperglycemic/hypoglycemic rats.
3 BiotechMesenchymal Stem Cell-Based Therapy for Diabetes Mellitus: Enhancement Strategies and Future Perspectives.
Stem cell reviews and reportsHealth-Related Quality of Life and Associated Factors Among Type Two Diabetic Patients on Follow-Up in Dessie Comprehensive Specialized Hospital, Dessie, North East Ethiopia, 2020.
Diabetes, metabolic syndrome and obesity : targets and therapyHypergonadotrophic hypogonadism in a patient with transaldolase deficiency: novel mutation in the pentose phosphate pathway.
Hormones (Athens, Greece)Fanconi-Bickel Syndrome: A Review of the Mechanisms That Lead to Dysglycaemia.
International journal of molecular sciencesA founder noncoding GALT variant interfering with splicing causes galactosemia.
Journal of inherited metabolic diseaseDiabetic ketoacidosis in a buck: a case report.
Iranian journal of veterinary researchSystemic AAV8-mediated delivery of a functional copy of muscle glycogen phosphorylase (Pygm) ameliorates disease in a murine model of McArdle disease.
Human molecular geneticsThe ability of an LC-MS/MS-based erythrocyte GALT enzyme assay to predict the phenotype in subjects with GALT deficiency.
Molecular genetics and metabolismValidation of an automated ultraperformance liquid chromatography IgG N-glycan analytical method applicable to classical galactosaemia.
Annals of clinical biochemistryClinical and biochemical heterogeneity between patients with glycogen storage disease type IA: the added value of CUSUM for metabolic control.
Journal of inherited metabolic disease[The analysis of level of total immunoglobulin E (IgE) in blood serum of patients with various types of disorders of carbohydrate metabolism and blood groups 0 (I), A (II) and B (III).].
Klinicheskaia laboratornaia diagnostikaA Fanconi-Bickel syndrome patient with a novel mutation and accompanying situs inversus totalis.
The Turkish journal of pediatricsImpaired glucose tolerance in Fanconi-Bickel syndrome: Eight patients with two novel mutations.
The Turkish journal of pediatricsThe Introduction of Submitted Approaches in Iranian Traditional Medicine for Treatment of Diabetes.
Iranian journal of medical sciencesFanconi Bickel Syndrome with Hypercalciuria due to GLUT 2 Mutation.
Indian pediatricsClassical Galactosaemia and CDG, the N-Glycosylation Interface. A Review.
JIMD reportsClassical galactosaemia: novel insights in IgG N-glycosylation and N-glycan biosynthesis.
European journal of human genetics : EJHG[Kidney diseases and metabolic disorders-Basics and applications required for general physicians. Topics: II. Disorder of carbohydrate metabolism].
Nihon Naika Gakkai zasshi. The Journal of the Japanese Society of Internal MedicineIgG N-Glycosylation Galactose Incorporation Ratios for the Monitoring of Classical Galactosaemia.
JIMD reports[SLC2A2 gene analysis in three Chinese children with Fanconi-Bickel syndrome].
Zhongguo dang dai er ke za zhi = Chinese journal of contemporary pediatricsAssociações
Organizações que acompanham esta doença — pra ter apoio e orientação
Ainda não temos associações cadastradas para Doença do metabolismo dos carboidratos.
É de uma associação que acompanha esta doença? Fale com a gente →
Comunidades
Grupos ativos de quem convive com esta doença aqui no Raras
Ainda não existe comunidade no Raras para Doença do metabolismo dos carboidratos
Pacientes, familiares e cuidadores se organizam em comunidades pra compartilhar experiências, fazer perguntas e se apoiar. Você pode ser o primeiro.
Tire suas dúvidas
Perguntas, dicas e experiências compartilhadas aqui na página
Participe da discussão
Faça login para postar dúvidas, compartilhar experiências e interagir com especialistas.
Fazer loginDoenças relacionadas
Doenças com sintomas parecidos — ajudam quem ainda está buscando diagnóstico
Referências e fontes
Bases de dados externas citadas neste artigo
Publicações científicas
Artigos indexados no PubMed ligados a esta doença no grafo RarasNet — título, periódico e PMID direto da fonte, sem intermediação de IA.
- Untargeted Proteomics Profiling of Liver and Plasma in Fed and Fasted Liver-Specific Glycogen Storage Disease Type Ia (GSD Ia) Mice: Toward Potential Protein Biomarkers.
- A 2-year-old girl with merged phenotypes: galactosemia and Coffin-Lowry syndrome.
- Neuromuscular pathology and mitochondrial dysfunction in sorbitol dehydrogenase gene-related distal hereditary motor neuropathies.
- A machine learning model accurately identifies glycogen storage disease Ia patients based on plasma acylcarnitine profiles.
- Multiomics approach provides insight into altered choline metabolism and liver injury in patients with glycogen storage disease type Ia.
Bases de dados e fontes oficiais
Identificadores e referências canônicas usadas para montar este verbete.
- ORPHA:79161(Orphanet)
- MONDO:0019214(MONDO)
- GARD:18946(GARD (NIH))
- Variantes catalogadas(ClinVar)
- Busca completa no PubMed(PubMed)
- Q18552029(Wikidata)
Dados compilados pelo RarasNet a partir de fontes abertas (Orphanet, OMIM, MONDO, PubMed/EuropePMC, ClinicalTrials.gov, DATASUS, PCDT/MS). Este conteúdo é informativo e não substitui avaliação médica.
Conteúdo mantido por Agente Raras · Médicos e pesquisadores podem colaborar
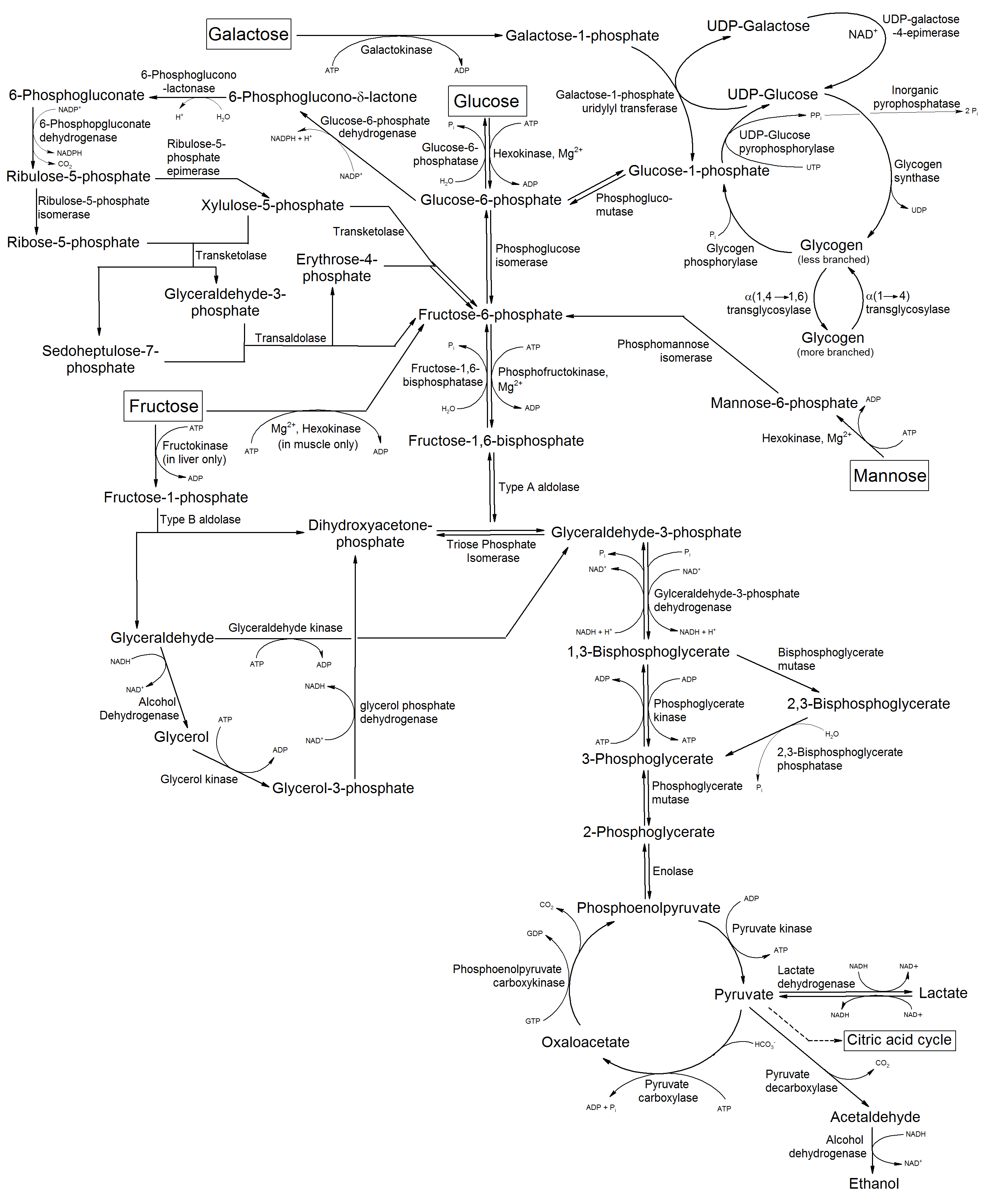
Doença do metabolismo dos carboidratos
📋 Origem dos dados
Esta página agrega dados de fontes públicas e oficiais. Dados sobre cobertura no SUS (PCDT, CEAF) são verificados ativamente por agente proativo (ver badge no infobox). Demais dados têm atribuição de fonte + data da última sincronização — clique para abrir o original.
- Doença rara (ontologia)
- fonte: Orphanet
- Identificador unificado
- fonte: MONDO
- Codificação WHO/SUS
- fonte: WHO ICD-10 / DATASUS
- NIH/GARD
- fonte: GARD (NIH)
- Indexação biomédica
- fonte: MeSH (NLM)
- Dado público estruturado
- fonte: Wikidata
- Ensaios clínicos
- fonte: ClinicalTrials.gov