A trissomia 16 em mosaico é uma síndrome cromossômica rara com características que variam muito, desde pequenas alterações com desenvolvimento normal até a morte neonatal. Pode causar atraso no crescimento do bebê na barriga da mãe, manchas na pele, assimetria do rosto e corpo, problemas no coração (como um "buraco" entre as cavidades, chamado defeito do septo ventricular) e nos órgãos genitais (como a uretra no lugar errado, chamada hipospadia, ou testículos que não descem, chamada criptorquidia), escoliose e perda auditiva. Outras características observadas incluem malformações esqueléticas (como dedos tortos ou extras, e pé torto), características faciais levemente diferentes e atraso no desenvolvimento.
Introdução
O que você precisa saber de cara
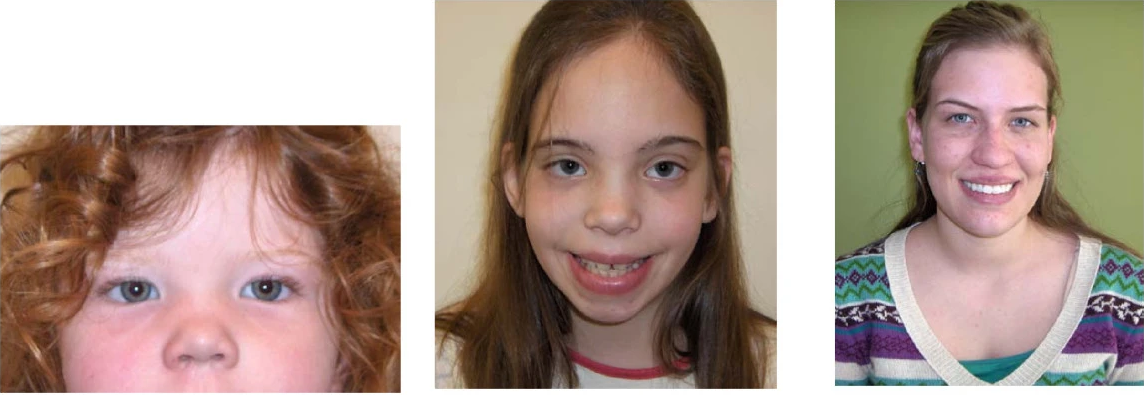
A trissomia 16 em mosaico é uma síndrome cromossômica rara com características que variam muito, desde pequenas alterações com desenvolvimento normal até a morte neonatal. Pode causar atraso no crescimento do bebê na barriga da mãe, manchas na pele, assimetria do rosto e corpo, problemas no coração (como um "buraco" entre as cavidades, chamado defeito do septo ventricular) e nos órgãos genitais (como a uretra no lugar errado, chamada hipospadia, ou testículos que não descem, chamada criptorquidia), escoliose e perda auditiva. Outras características observadas incluem malformações esqueléticas (como dedos tortos ou extras, e pé torto), características faciais levemente diferentes e atraso no desenvolvimento.
Escala de raridade
<1/50kMuito rara
1/20kRara
1/10kPouco freq.
1/5kIncomum
1/2k
Encontrou um erro ou informação desatualizada? Sugira uma correção →
Entender a doença
Do básico ao detalhe, leia no seu ritmo
Preparando trilha educativa...
Sinais e sintomas
O que aparece no corpo e com que frequência cada sintoma acontece
Partes do corpo afetadas
+ 15 sintomas em outras categorias
Características mais comuns
Os sintomas variam de pessoa para pessoa. Abaixo estão as 43 características clínicas mais associadas, ordenadas por frequência.
Linha do tempo da pesquisa
Encontrou um erro ou informação desatualizada? Sugira uma correção →
Genética e causas
O que está alterado no DNA e como passa nas famílias
Condição cromossômica — cromossomo 16
Causada pelo excesso de material do cromossomo 16. O fenótipo resulta da alteração na dose de múltiplos genes simultaneamente — não há gene causal único. Diagnóstico por cariótipo, CMA ou FISH.
Genes triplosensíveis (sensíveis ao excesso de dose)
Genes do cromossomo 16 com evidência de sensibilidade à dose segundo ClinGen Dosage Map . São fortes candidatos a explicar parte do fenótipo (1 ao todo).
Fontes: ClinGen Dosage Sensitivity Map · GENCODE v44 (GRCh38)
Diagnóstico
Os sinais que médicos procuram e os exames que confirmam
Tratamento e manejo
Remédios, cuidados de apoio e o que precisa acompanhar
Onde tratar no SUS
Hospitais de referência no Brasil e o protocolo oficial do SUS (PCDT)
🇧🇷 Atendimento SUS — Trissomia 16 em mosaico
Selecione um estado ou use sua localização para ver resultados.
Dados de DATASUS/CNES, SBGM, ABNeuro e Ministério da Saúde. Sempre confirme a disponibilidade diretamente com o estabelecimento.
Pesquisa ativa
Ensaios clínicos abertos e novidades científicas recentes
Pesquisa e ensaios clínicos
Nenhum ensaio clínico registrado para esta condição.
Publicações mais relevantes
Clinical and Molecular Presentation of a Patient with Paternal Uniparental Isodisomy of Chromosome 16.
Uniparental disomies (UPDs) are among the causes of imprinting disorders. Specific phenotypes of most causative UPDs have been described. Here, we describe the case of a 2-year-old female patient who presented a syndromic phenotype. Chromosomal microarray analysis revealed UPD of the whole chromosome 16. Microsatellite analysis demonstrated paternal origin of the UPD and its isodisomic pattern (UPiD (16) pat). Mosaic trisomy 16 was not detected using the FISH method. Whole-exome sequencing revealed no pathogenetic genetic variants sufficient to explain the syndromic phenotype nor unmasked pathogenic recessive genetic variants on chromosome 16. Whole-genome trio DNA sequencing revealed no additional candidate pathogenic genetic variants to those detected by whole-exome sequencing, including miRNAs and lncRNAs. Imprinting disorders at 6q24.2, 7p12.2, 7q32.2, 11p15.5, 14q32.2, 15q11.2, and 20q13.32, as well as multilocus imprinting disturbances (MLIDs), were excluded by Methylation-Specific Multiplex Ligation-Dependent Probe Amplification (MS-MLPA). At the same time, we detected abnormal hypermethylation of the ZNF597 transcription start site differentially methylated region (ZNF597:TSS-DMR), accompanied by hypomethylation of the neighbouring ZNF597:3' DMR. Both DMRs were normally imprinted, and the DNA alterations in our patient with UPD (16) pat are opposite to those previously described for maternal uniparental disomy (UPD (16) mat). To date, several cases of UPD (16) pat have been reported. Our case report describes the syndromic phenotype of a patient with paternal uniparental disomy of chromosome 16 in contrast to the previously described patients with a normal phenotype or with abnormal phenotypes caused by acquired homozygosity of pathogenic variants at autosomal recessive genes located on this chromosome. Reporting such observations will help systematize data on the phenotypes of imprinting disorders on chromosome 16.
Co-Occurrence of Urogenital Anomalies and Congenital Heart Disease in a Child With Alpha-Thalassemia Mental Retardation Syndrome Associated With Chromosome 16 Abnormalities due to Partial Monosomy 16p13.3 and Partial Trisomy 16q22.1-q24.3.
We report the case of a 3-year-old girl with alpha-thalassemia/mental retardation linked to chromosome 16 (ATR-16) syndrome. The patient presented with hypotonia, developmental delay, and characteristic facial features including hypertelorism and a broad nasal bridge. Blood test results indicated microcytic anemia and normal iron status, suggestive of thalassemia. Genetic analysis revealed that the patient harbored a 465 kb deletion in the 16p13.3 region and a 19.4 Mb duplication in the 16q22.1-q24.3 region. The patient presented with rare complications of ATR-16 syndrome, including anal fistula, vesicoureteral reflux (VUR), and patent ductus arteriosus (PDA). Comparison of this case with previously reported patients with pure partial trisomy 16q suggested that the duplicated distal 16q region may be a critical locus associated with VUR and PDA.
Cell-type-specific enrichment of somatic aneuploidy in the mammalian brain.
Somatic mutations alter the genomes of a subset of an individual's brain cells, impacting gene regulation and contributing to disease processes. Mosaic single-nucleotide variants have been characterized with single-cell resolution in the brain, but we have limited information about large-scale structural variation such as whole-chromosome duplication or loss. We used a dataset of over 415,000 single-cell DNA methylation and chromatin conformation profiles from the adult mouse brain to comprehensively identify and characterize aneuploid cells. Somatic trisomy events were strongly enriched on chromosome 16, which is syntenic with human chromosome 21. We also observed a specific enrichment of chromosome gain and loss events in specific cell types, including Pons neurons and oligodendrocyte precursor cells. Chromosome 16 trisomy occurred in multiple cell types and across brain regions, suggesting that nondisjunction is a recurrent feature of somatic structural variation in the brain.
Limited additional value of karyotyping cultured amniotic fluid cell colonies in addition to microarray on uncultured cells for confirmation of abnormal non-invasive prenatal testing results.
Non-invasive prenatal testing (NIPT) allows the detection of placental chromosome aberrations. To verify whether the fetus also has the chromosome aberration, diagnostic follow-up testing is required. The aim of this retrospective study was to assess the added value of analyzing amniotic fluid (AF) cell cultures in addition to uncultured AF cells for the detection of fetal mosaicism. NIPT was performed as part of the Dutch TRIDENT study. Cytogenetic studies in uncultured AF were performed using single nucleotide polymorphism (SNP)-array. Cultured AF cell colonies (in situ method) were investigated with fluorescent in situ hybridization and/or karyotyping. Clinical outcome data were collected in cases with discordant results. Between April 2014 and December 2021, 368 amniocenteses were performed after a chromosomal aberration was detected with NIPT. Excluding 134 cases of common aneuploidies (confirmed by quantitative fluorescence polymerase chain reaction), 29 cases with investigation of uncultured cells only and 1 case without informed consent, 204 cases were eligible for this study. In 196 (96%) cases, the results in uncultured and cultured cells were concordant normal, abnormal or mosaic. Five cases (2%) showed mosaicism in cultured AF cells, whereas uncultured AF cells were normal. Two (1%) of these, one mosaic trisomy 13 and one mosaic trisomy 16, were considered true fetal mosaics. The added value of investigating AF cell cultures in addition to uncultured cells is limited to two of 204 (1%) cases in which true fetal mosaicsm would otherwise be missed. The clinical relevance of one (trisomy 13) remained unknown and the other case also showed ultrasound anomalies, which determined pregnancy management. This seems to justify limiting prenatal cytogenetic confirmatory testing to SNP arrays on uncultured AF cells, considerably shortening the reporting time.
Generation of functional oocytes from male mice in vitro.
Sex chromosome disorders severely compromise gametogenesis in both males and females. In oogenesis, the presence of an additional Y chromosome or the loss of an X chromosome disturbs the robust production of oocytes1-5. Here we efficiently converted the XY chromosome set to XX without an additional Y chromosome in mouse pluripotent stem (PS) cells. In addition, this chromosomal alteration successfully eradicated trisomy 16, a model of Down's syndrome, in PS cells. Artificially produced euploid XX PS cells differentiated into mature oocytes in culture with similar efficiency to native XX PS cells. Using this method, we differentiated induced pluripotent stem cells from the tail of a sexually mature male mouse into fully potent oocytes, which gave rise to offspring after fertilization. This study provides insights that could ameliorate infertility caused by sex chromosome or autosomal disorders, and opens the possibility of bipaternal reproduction.
Publicações recentes
Clinical and Molecular Presentation of a Patient with Paternal Uniparental Isodisomy of Chromosome 16.
Endocrine Abnormalities in Mosaic Trisomy 16 Adolescent: A Case Report.
Limited additional value of karyotyping cultured amniotic fluid cell colonies in addition to microarray on uncultured cells for confirmation of abnormal non-invasive prenatal testing results.
Mosaic trisomy 16 at amniocentesis in a pregnancy associated with positive non-invasive prenatal testing for trisomy 16, placental trisomy 16, intrauterine growth restriction, intrauterine fetal death, cytogenetic discrepancy between cultured amniocytes and uncultured amniocytes, and prenatal progressive decrease of the aneuploid cell line.
Characteristics and mechanisms of mosaicism in prenatal diagnosis cases by application of SNP array.
📚 EuropePMCmostrando 14
Co-Occurrence of Urogenital Anomalies and Congenital Heart Disease in a Child With Alpha-Thalassemia Mental Retardation Syndrome Associated With Chromosome 16 Abnormalities due to Partial Monosomy 16p13.3 and Partial Trisomy 16q22.1-q24.3.
Congenital anomaliesClinical and Molecular Presentation of a Patient with Paternal Uniparental Isodisomy of Chromosome 16.
International journal of molecular sciencesCell-type-specific enrichment of somatic aneuploidy in the mammalian brain.
NeuronCell type-specific enrichment of somatic aneuploidy in the mammalian brain.
bioRxiv : the preprint server for biologyLimited additional value of karyotyping cultured amniotic fluid cell colonies in addition to microarray on uncultured cells for confirmation of abnormal non-invasive prenatal testing results.
Prenatal diagnosisGeneration of functional oocytes from male mice in vitro.
NaturePrenatal diagnosis of mosaic trisomy 16 by amniocentesis in a pregnancy associated with abnormal first-trimester screening result (low PAPP-A and low PlGF), intrauterine growth restriction and a favorable outcome.
Taiwanese journal of obstetrics & gynecology[Comparison of the etiological constitution of two and three or more recurrent miscarriage].
Zhonghua fu chan ke za zhiPrenatal diagnosis and molecular cytogenetic characterization of mosaicism for a small supernumerary marker chromosome derived from chromosome 16.
Taiwanese journal of obstetrics & gynecologyKnockdown of Myo-Inositol Transporter SMIT1 Normalizes Cholinergic and Glutamatergic Function in an Immortalized Cell Line Established from the Cerebral Cortex of a Trisomy 16 Fetal Mouse, an Animal Model of Human Trisomy 21 (Down Syndrome).
Neurotoxicity research[Comprehensive Analyses of Molecules with Altered Expression in the Brain of a Mouse Model of Down Syndrome for Identification of Pharmacotherapeutic Targets].
Yakugaku zasshi : Journal of the Pharmaceutical Society of JapanTs1Cje Down syndrome model mice exhibit environmental stimuli-triggered locomotor hyperactivity and sociability concurrent with increased flux through central dopamine and serotonin metabolism.
Experimental neurologyAbsence of Prenatal Forebrain Defects in the Dp(16)1Yey/+ Mouse Model of Down Syndrome.
The Journal of neuroscience : the official journal of the Society for NeuroscienceRestrained Phosphatidylcholine Synthesis in a Cellular Model of Down's Syndrome is Associated with the Overexpression of Dyrk1A.
Molecular neurobiologyAssociações
Organizações que acompanham esta doença — pra ter apoio e orientação
Ainda não temos associações cadastradas para Trissomia 16 em mosaico.
É de uma associação que acompanha esta doença? Fale com a gente →
Comunidades
Grupos ativos de quem convive com esta doença aqui no Raras
Ainda não existe comunidade no Raras para Trissomia 16 em mosaico
Pacientes, familiares e cuidadores se organizam em comunidades pra compartilhar experiências, fazer perguntas e se apoiar. Você pode ser o primeiro.
Tire suas dúvidas
Perguntas, dicas e experiências compartilhadas aqui na página
Participe da discussão
Faça login para postar dúvidas, compartilhar experiências e interagir com especialistas.
Fazer loginDoenças relacionadas
Doenças com sintomas parecidos — ajudam quem ainda está buscando diagnóstico
Referências e fontes
Bases de dados externas citadas neste artigo
Publicações científicas
Artigos indexados no PubMed ligados a esta doença no grafo RarasNet — título, periódico e PMID direto da fonte, sem intermediação de IA.
- Clinical and Molecular Presentation of a Patient with Paternal Uniparental Isodisomy of Chromosome 16.
- Co-Occurrence of Urogenital Anomalies and Congenital Heart Disease in a Child With Alpha-Thalassemia Mental Retardation Syndrome Associated With Chromosome 16 Abnormalities due to Partial Monosomy 16p13.3 and Partial Trisomy 16q22.1-q24.3.
- Cell-type-specific enrichment of somatic aneuploidy in the mammalian brain.
- Limited additional value of karyotyping cultured amniotic fluid cell colonies in addition to microarray on uncultured cells for confirmation of abnormal non-invasive prenatal testing results.
- Generation of functional oocytes from male mice in vitro.
- Endocrine Abnormalities in Mosaic Trisomy 16 Adolescent: A Case Report.
- Mosaic trisomy 16 at amniocentesis in a pregnancy associated with positive non-invasive prenatal testing for trisomy 16, placental trisomy 16, intrauterine growth restriction, intrauterine fetal death, cytogenetic discrepancy between cultured amniocytes and uncultured amniocytes, and prenatal progressive decrease of the aneuploid cell line.
- Characteristics and mechanisms of mosaicism in prenatal diagnosis cases by application of SNP array.
Bases de dados e fontes oficiais
Identificadores e referências canônicas usadas para montar este verbete.
- ORPHA:1708(Orphanet)
- MONDO:0015729(MONDO)
- GARD:18741(GARD (NIH))
- Busca completa no PubMed(PubMed)
- Artigo Wikipedia(Wikipedia)
- Q503642(Wikidata)
Dados compilados pelo RarasNet a partir de fontes abertas (Orphanet, OMIM, MONDO, PubMed/EuropePMC, ClinicalTrials.gov, DATASUS, PCDT/MS). Este conteúdo é informativo e não substitui avaliação médica.
Conteúdo mantido por Agente Raras · Médicos e pesquisadores podem colaborar
Trissomia 16 em mosaico
📋 Origem dos dados
Esta página agrega dados de fontes públicas e oficiais. Dados sobre cobertura no SUS (PCDT, CEAF) são verificados ativamente por agente proativo (ver badge no infobox). Demais dados têm atribuição de fonte + data da última sincronização — clique para abrir o original.
- Doença rara (ontologia)
- fonte: Orphanet
- Identificador unificado
- fonte: MONDO
- Codificação WHO/SUS
- fonte: WHO ICD-10 / DATASUS
- CID-11 (futuro)
- fonte: WHO ICD-11
- NIH/GARD
- fonte: GARD (NIH)
- Indexação biomédica
- fonte: MeSH (NLM)
- Dado público estruturado
- fonte: Wikidata