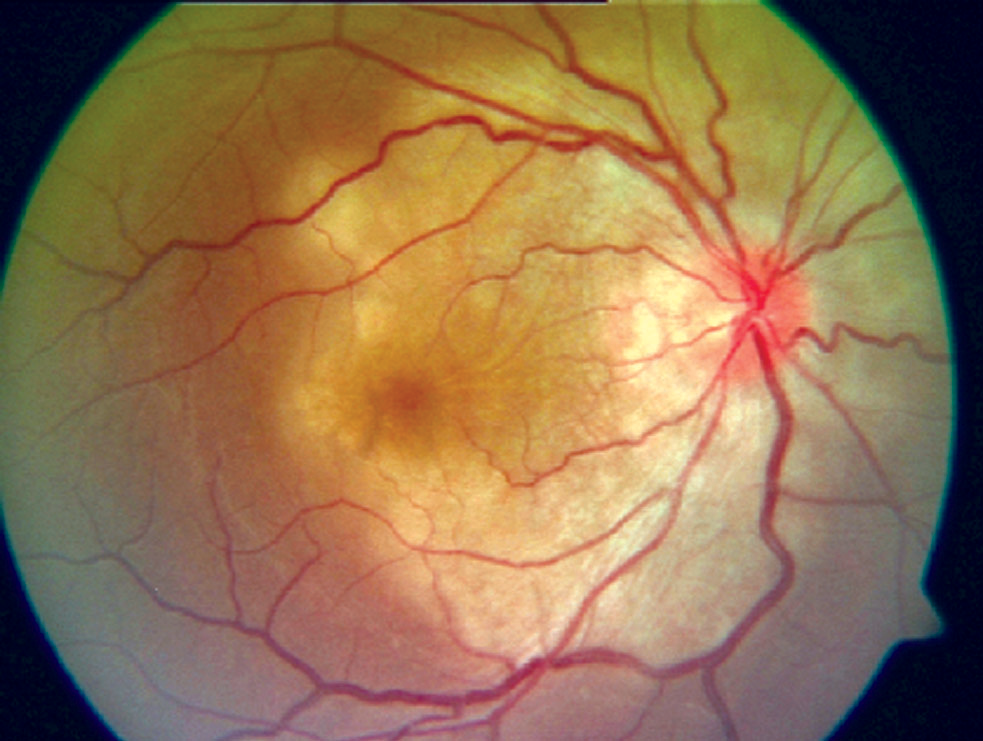
A maculopatia placóide persistente é uma condição caracterizada por lesões brancas, em forma de placa, que surgem na mácula (a área central da retina, responsável pela visão de detalhes), mas não afetam a região ao redor do nervo óptico em ambos os olhos. Até o momento, foi descrita em apenas cinco pacientes. Ao contrário de pacientes com uma condição similar chamada coroidite serpiginosa macular, que também mostram lesões parecidas, os cinco pacientes com maculopatia placóide persistente mantiveram uma boa visão até o surgimento de neovascularização da coroide (NVC – que é a formação de novos vasos sanguíneos anormais) ou o aparecimento de manchas e alterações na pigmentação. As lesões na mácula tendem a desaparecer após alguns meses ou anos, mas as alterações nos vasos sanguíneos persistem, o que acaba levando à perda da visão central.
Introdução
O que você precisa saber de cara
A maculopatia placóide persistente é uma condição caracterizada por lesões brancas, em forma de placa, que surgem na mácula (a área central da retina, responsável pela visão de detalhes), mas não afetam a região ao redor do nervo óptico em ambos os olhos. Até o momento, foi descrita em apenas cinco pacientes. Ao contrário de pacientes com uma condição similar chamada coroidite serpiginosa macular, que também mostram lesões parecidas, os cinco pacientes com maculopatia placóide persistente mantiveram uma boa visão até o surgimento de neovascularização da coroide (NVC – que é a formação de novos vasos sanguíneos anormais) ou o aparecimento de manchas e alterações na pigmentação. As lesões na mácula tendem a desaparecer após alguns meses ou anos, mas as alterações nos vasos sanguíneos persistem, o que acaba levando à perda da visão central.
Escala de raridade
<1/50kMuito rara
1/20kRara
1/10kPouco freq.
1/5kIncomum
1/2k
Encontrou um erro ou informação desatualizada? Sugira uma correção →
Entender a doença
Do básico ao detalhe, leia no seu ritmo
Preparando trilha educativa...
Sinais e sintomas
O que aparece no corpo e com que frequência cada sintoma acontece
Partes do corpo afetadas
+ 3 sintomas em outras categorias
Características mais comuns
Os sintomas variam de pessoa para pessoa. Abaixo estão as 8 características clínicas mais associadas, ordenadas por frequência.
Linha do tempo da pesquisa
Encontrou um erro ou informação desatualizada? Sugira uma correção →
Genética e causas
O que está alterado no DNA e como passa nas famílias
Nenhum gene associado encontrado
Os dados genéticos desta condição ainda estão sendo catalogados.
Diagnóstico
Os sinais que médicos procuram e os exames que confirmam
Tratamento e manejo
Remédios, cuidados de apoio e o que precisa acompanhar
Onde tratar no SUS
Hospitais de referência no Brasil e o protocolo oficial do SUS (PCDT)
🇧🇷 Atendimento SUS — Maculopatia placóide persistente
Selecione um estado ou use sua localização para ver resultados.
Dados de DATASUS/CNES, SBGM, ABNeuro e Ministério da Saúde. Sempre confirme a disponibilidade diretamente com o estabelecimento.
Pesquisa ativa
Ensaios clínicos abertos e novidades científicas recentes
Pesquisa e ensaios clínicos
Nenhum ensaio clínico registrado para esta condição.
Publicações mais relevantes
NON-INFECTIOUS POSTERIOR UVEITIDES - Atypicals, Variants, and Masquerades: the jungle of differential diagnosis.
Non-infectious posterior and panuveitides (NIPUs) comprise a heterogeneous group of inflammatory disorders of the outer retina and choroid, historically referred to as "white dot syndromes." Recent consensus efforts by the Multimodal Imaging in Uveitis (MUV) Task Force have established standardized diagnostic criteria for the major NIPUs, including multiple evanescent white dot syndrome (MEWDS), multifocal choroiditis and panuveitis/punctate inner choroiditis (MFCPU/PIC), acute posterior multifocal placoid pigment epitheliopathy (APMPPE), serpiginous choroiditis, and birdshot chorioretinopathy (BSCR). Nevertheless, a substantial proportion of cases deviate from classical presentations and fall into diagnostic "grey zones", blurring boundaries between diseases entities and complicating both differential diagnosis and management. This review aims to describe the broad spectrum of atypical, variant, and secondary forms of NIPUs as well as masquerade syndromes. Atypical MEWDS includes bilateral presentations or complicated courses, while MFCPU/PIC with outer retinal atrophy emerges as a notable entity with unclear therapeutic implications. Inflammatory reactions resembling both MEWDS and MFCPU/PIC may also occur as secondary phenomena, triggered by other chorioretinal disorders, most notably inherited retinal diseases (IRDs). Placoid chorioretinopathies, including APMPPE, persistent placoid maculopathy, serpiginous choroiditis, and relentless placoid chorioretinitis, are often distinguished only a posteriori based on disease course, but likely represent a continuum of disorders unified by choroidal ischemia. Atypical presentations of BSCR may feature extensive outer retinal damage, mimicking IRDs. Equally important is the consideration of masquerade syndromes in all suspected cases of NIPUs, as they can present with similar features yet require entirely different treatments. Infectious masquerades include tuberculosis-associated serpiginous-like choroiditis, acute syphilitic posterior placoid chorioretinopathy, and West Nile virus chorioretinitis, whereas vitreoretinal lymphoma is the most frequent neoplastic masquerade. In conclusion, integrating clinical context with high-quality multimodal imaging remains essential to navigate the jungle of differential diagnosis in NIPUs, while future studies should aim to link imaging phenotypes with immune and molecular biomarkers to refine classification and guide targeted therapies.
Clinical and Imaging Features Aiding the Differentiation of Acute Posterior Multifocal Placoid Pigmented Epitheliopathy from Other Placoid Diseases.
To describe clinical and multimodal imaging features of patients with Acute Posterior Multifocal Placoid Pigmented Epitheliopathy (APMPPE) and identify distinctive characteristics guiding in the differentiation between APMPPE and other placoid conditions (non-APMPPE). Retrospective single-center observational study of all patients diagnosed with APMPPE in the Uveitis Service of Moorfields Eye Hospital between 2002 and 2022. Sixty patients with presumed APMPPE at presentation were included, of whom 37 had a confirmed diagnosis of APMPPE, and 23 received a different diagnosis (non-APMPPE) during the follow-up. Non-APMPPE included ampiginous choroiditis (6 patients), idiopathic multifocal choroiditis (5 patients), tubercular multifocal choroiditis (5 patients), serpiginous choroiditis (1 patient), tubercular serpiginous-like choroiditis (3 patients), sarcoidosis (2 patients) and persistent placoid maculopathy (1 patient). Compared to non-APMPPE, APMPPE was more commonly observed in individuals of white ethnicity (p = 0.025), had shorter duration of symptoms (11.3 days, p = 0.02) and was associated with a viral prodrome (p < 0.001). APMPPE course was more commonly non-relapsing compared to non-APMPPE (p = 0.02), although relapses were observed in 18.9% of APMPPE cases. Mean final BCVA was significantly better in the APMPPE group (p = 0.04). Subfoveal choroidal thickness at presentation and final visit was significantly greater in APMPPE compared to non-APMPPE (p < 0.001), both in the eyes affected and fellow eyes that became affected later. In addition to the established clinical features and multimodal imaging characteristics, ethnicity, duration of symptoms, viral prodrome and subfoveal choroidal thickness can add useful information in guiding physicians in differentiating APMPPE from other mimicking placoid conditions.
Different clinical presentations of persistent placoid maculopathy: a case series.
Persistent placoid maculopathy is a rare clinical entity defined as idiopathic bilateral chorioretinopathy. We report four different clinical presentations of this pathology. Case 1: A 63-year-old man presented with a persistent bilateral central scotoma. Persistent placoid maculopathy was diagnosed based on ophthalmological manifestations and multimodal imaging. A history of scalp tenderness and jaw claudication a week before visual symptoms was reported associated with increased C-reactive protein. A temporal artery biopsy confirmed the diagnosis of giant cell arteritis. Despite corticosteroid treatment, complete macular chorioretinal atrophy followed. Case 2: A 65-year-old woman was referred for bilateral blurred vision for one month. Visual acuity was 20/20 in both eyes and multimodal imaging confirmed the diagnosis of persistent placoid maculopathy. The patient was lost to follow-up due to the COVID-19 pandemic and presented one year later with decreased vision in the left eye of 20/200. Type 2 choroidal neovascularization was observed and treated with sub-tenon triamcinolone injection followed by intravitreal injection of Aflibercept allowing an improvement in visual acuity. Case 3: A 61-year-old man presented with sudden loss of vision in his right eye. A large submacular hemorrhage was observed on the right eye and hypopigmented white/yellowish plaque-like macular lesions on the other eye. Surgery with pneumatic displacement and intravitreal injection of Aflibercept was performed. No improvement in visual acuity was observed. Five months later, the contralateral eye was complicated by choroidal neovascularization and required intravitreal injections. Case 4: A 49-year-old man receiving immunosuppressive therapy after liver transplant was referred for bilateral decreased vision. The diagnosis of persistent placoid maculopathy was made, and corticosteroid treatment was initiated. After three months, chorioretinal lesions decreased and vision recovered. We report the first case series of clinical presentations of persistent placoid maculopathy, which expand upon the reported ocular manifestations of this condition.
ACUTE POSTERIOR MULTIFOCAL PLACOID PIGMENT EPITHELIOPATHY AND PLACOID VARIANT DISEASES MASQUERADING AS AGE-RELATED MACULAR DEGENERATION IN THE ELDERLY: A Case Series.
To report eight cases of acute posterior multifocal placoid pigment epitheliopathy (APMPPE) or persistent placoid maculopathy (PPM) initially masquerading as age-related macular degeneration in elderly individuals. APMPPE or PPM eyes in patients above age 55 years with macular retinal pigment epithelium disruption including drusenoid lesions on macular examination and/or with multimodal imaging were included. At least one method of multimodal imaging including fluorescein angiography (FA), indocyanine green angiography, optical coherence tomography (OCT), and OCT angiography (OCTA) was performed in all eyes for diagnosis and to monitor for macular neovascularization. Eight elderly male patients presented with vision loss and were all initially diagnosed with non-neovascular or neovascular age-related macular degeneration. With the aid of multimodal retinal imaging, a final diagnosis of either APMPPE or PPM was rendered. With FA and indocyanine green angiography, choroidal hypoperfusion was detected in all but one eye. With OCT, the angular sign of Henle fiber layer hyperreflectivity was identified in >50% of eyes. With OCTA, inner choroidal flow deficits were detected in all eyes. Macular neovascularization requiring anti-vascular endothelial growth factor injection therapy complicated three of eight cases. Both APMPPE and PPM may develop in elderly individuals and may masquerade as age-related macular degeneration on presentation. Multimodal imaging including FA, indocyanine green angiography, and OCTA are important diagnostic modalities to assess for inner choroidal hypoperfusion to arrive at an accurate diagnosis and to detect macular neovascularization, which frequently complicates APMPPE and PPM. In these patients, serial anti-vascular endothelial growth factor intravitreal injections are essential in treating macular neovascularization and in preventing significant vision loss.
Persistent Placoid Maculopathy: Lichen-like Lesions Growing between Retinal Pigment Epithelium and Bruch's Membrane.
To report the novel imaging findings in persistent placoid maculopathy (PPM) from the first case series of Asian subjects. Retrospective observational case series. Patients with PPM from 2013 to 2023. Medical records and multimodal images from each visit were analyzed. Imaging and follow-up findings. Twenty-one eyes of 16 patients were included. Mean age was 61 (range, 48-84) years old. Five patients showed bilateral involvement. Persistent placoid maculopathy lesions were unremarkable on color fundus photography, autofluorescence, and fluorescein angiography. Hypofluorescent spots with a lichen-like appearance presented in all phases of indocyanine green angiography, which were most prominent in the late phase and presented in a fused (71%) or clustered (29%) pattern. The hypofluorescence correlated with the lesions between the retinal pigment epithelium (RPE) and Bruch's membrane (BM) with moderate reflectivity on OCT, and the thickness ranged from slit-like to mound-like. The intensity of hypofluorescence sometimes varied in the same eye and correlated with the thickness of sub-RPE lesions on OCT. No abnormal blood flow signals were detected in either the sub-RPE space or choriocapillaris slab of OCT angiography across the PPM lesions. Peripapillary (5 eyes, 24%) and extra posterior pole (2 eyes, 10%) involvements were seen, the former sparing the β zones of optic discs. Ten eyes of 7 patients were followed up (median, 26 months; range, 2-121 months). During follow-up, the lichen-like lesions spread and migrated slowly without changing the plane patterns of the first visit and were limited to sub-RPE growth. The fused lichen-like pattern sprawled around the enlarged base. The clustered lichen-like pattern gradually loosened. Ten eyes (48%, 9 eyes in the fused pattern, 1 eye in the clustered pattern) had secondary choroidal neovascularization (CNV) at the first visit, with type I (6 eyes, 5 of which were polypoidal choroidal vasculopathy) and type II (4 eyes). No new CNV developed during follow-up. Persistent placoid maculopathy lesions were located in the sub-RPE space, as determined by multimodal imaging. Spreading and migration between the RPE and BM may account for their unique lichen-like appearance and progression pattern. Proprietary or commercial disclosure may be found in the Footnotes and Disclosures at the end of this article.
Publicações recentes
Noninfectious Posterior Uveitides - Atypicals, Variants, and Masquerades: The Jungle of Differential Diagnosis.
Clinical and Imaging Features Aiding the Differentiation of Acute Posterior Multifocal Placoid Pigmented Epitheliopathy from Other Placoid Diseases.
Different clinical presentations of persistent placoid maculopathy: a case series.
ACUTE POSTERIOR MULTIFOCAL PLACOID PIGMENT EPITHELIOPATHY AND PLACOID VARIANT DISEASES MASQUERADING AS AGE-RELATED MACULAR DEGENERATION IN THE ELDERLY: A Case Series.
Re: Li et al.: Persistent placoid maculopathy: lichen-like lesions growing between retinal pigment epithelium and Bruch's membrane (Ophthalmol Retina. 2024;8:270-278).
📚 EuropePMC23 artigos no totalmostrando 22
NON-INFECTIOUS POSTERIOR UVEITIDES - Atypicals, Variants, and Masquerades: the jungle of differential diagnosis.
American journal of ophthalmologyClinical and Imaging Features Aiding the Differentiation of Acute Posterior Multifocal Placoid Pigmented Epitheliopathy from Other Placoid Diseases.
Ocular immunology and inflammationDifferent clinical presentations of persistent placoid maculopathy: a case series.
BMC ophthalmologyACUTE POSTERIOR MULTIFOCAL PLACOID PIGMENT EPITHELIOPATHY AND PLACOID VARIANT DISEASES MASQUERADING AS AGE-RELATED MACULAR DEGENERATION IN THE ELDERLY: A Case Series.
Retina (Philadelphia, Pa.)Re: Li et al.: Persistent placoid maculopathy: lichen-like lesions growing between retinal pigment epithelium and Bruch's membrane (Ophthalmol Retina. 2024;8:270-278).
Ophthalmology. RetinaPersistent Placoid Maculopathy: Lichen-like Lesions Growing between Retinal Pigment Epithelium and Bruch's Membrane.
Ophthalmology. Retina[Acute posterior multifocal placoid pigment epitheliopathy, serpiginous choroiditis and related diseases].
Journal francais d'ophtalmologieLongitudinal quantification of choriocapillaris flow deficits in persistent placoid maculopathy: a case report.
BMC ophthalmologyBilateral Persistent Placoid Maculopathy Following COVID-19 Vaccines: Real or Coincidence?
Ocular immunology and inflammationChoroidal ischemia drives macular neovascularization in persistent placoid maculopathy.
American journal of ophthalmology case reportsPlacoid lesions of the retina: progress in multimodal imaging and clinical perspective.
The British journal of ophthalmologySevere persistent placoid maculopathy: Atypical presentation in a young male.
European journal of ophthalmologyPersistent Placoid Maculopathy: Prognosis Factors and Functional Outcomes.
Ocular immunology and inflammationPERSISTENT PLACOID MACULOPATHY-LIKE FINDINGS IN PATIENTS WITH GIANT CELL ARTERITIS.
Retinal cases & brief reportsComparison of choroidal neovascularization secondary to white dot syndromes and age-related macular degeneration by using optical coherence tomography angiography.
Clinical ophthalmology (Auckland, N.Z.)PERSISTENT PLACOID MACULOPATHY: A Systematic Review.
Retina (Philadelphia, Pa.)PERSISTENT PLACOID MACULOPATHY IN A PATIENT WITH HIGH MYOPIA.
Retinal cases & brief reportsChorioretinal Perfusion in Persistent Placoid Maculopathy.
Ophthalmic surgery, lasers & imaging retinaPersistent Placoid Maculopathy Complicated by Cerebral Vasculitis.
Journal of neuro-ophthalmology : the official journal of the North American Neuro-Ophthalmology SocietyOptical Coherence Tomography Angiography Reveals Choriocapillaris Flow Reduction in Placoid Chorioretinitis.
Ophthalmology. RetinaPERSISTENT PLACOID MACULOPATHY IMAGED BY OPTICAL COHERENCE TOMOGRAPHY ANGIOGRAPHY.
Retinal cases & brief reportsPATHOGENESIS OF PERSISTENT PLACOID MACULOPATHY: A Multimodal Imaging Analysis.
Retina (Philadelphia, Pa.)Associações
Organizações que acompanham esta doença — pra ter apoio e orientação
Ainda não temos associações cadastradas para Maculopatia placóide persistente.
É de uma associação que acompanha esta doença? Fale com a gente →
Comunidades
Grupos ativos de quem convive com esta doença aqui no Raras
Ainda não existe comunidade no Raras para Maculopatia placóide persistente
Pacientes, familiares e cuidadores se organizam em comunidades pra compartilhar experiências, fazer perguntas e se apoiar. Você pode ser o primeiro.
Tire suas dúvidas
Perguntas, dicas e experiências compartilhadas aqui na página
Participe da discussão
Faça login para postar dúvidas, compartilhar experiências e interagir com especialistas.
Fazer loginDoenças relacionadas
Doenças com sintomas parecidos — ajudam quem ainda está buscando diagnóstico
Referências e fontes
Bases de dados externas citadas neste artigo
Publicações científicas
Artigos indexados no PubMed ligados a esta doença no grafo RarasNet — título, periódico e PMID direto da fonte, sem intermediação de IA.
- NON-INFECTIOUS POSTERIOR UVEITIDES - Atypicals, Variants, and Masquerades: the jungle of differential diagnosis.
- Clinical and Imaging Features Aiding the Differentiation of Acute Posterior Multifocal Placoid Pigmented Epitheliopathy from Other Placoid Diseases.
- Different clinical presentations of persistent placoid maculopathy: a case series.
- ACUTE POSTERIOR MULTIFOCAL PLACOID PIGMENT EPITHELIOPATHY AND PLACOID VARIANT DISEASES MASQUERADING AS AGE-RELATED MACULAR DEGENERATION IN THE ELDERLY: A Case Series.
- Persistent Placoid Maculopathy: Lichen-like Lesions Growing between Retinal Pigment Epithelium and Bruch's Membrane.
- Re: Li et al.: Persistent placoid maculopathy: lichen-like lesions growing between retinal pigment epithelium and Bruch's membrane (Ophthalmol Retina. 2024;8:270-278).
Bases de dados e fontes oficiais
Identificadores e referências canônicas usadas para montar este verbete.
- ORPHA:97341(Orphanet)
- MONDO:0019973(MONDO)
- GARD:19369(GARD (NIH))
- Busca completa no PubMed(PubMed)
- Q55789022(Wikidata)
Dados compilados pelo RarasNet a partir de fontes abertas (Orphanet, OMIM, MONDO, PubMed/EuropePMC, ClinicalTrials.gov, DATASUS, PCDT/MS). Este conteúdo é informativo e não substitui avaliação médica.
Conteúdo mantido por Agente Raras · Médicos e pesquisadores podem colaborar
Maculopatia placóide persistente
📋 Origem dos dados
Esta página agrega dados de fontes públicas e oficiais. Dados sobre cobertura no SUS (PCDT, CEAF) são verificados ativamente por agente proativo (ver badge no infobox). Demais dados têm atribuição de fonte + data da última sincronização — clique para abrir o original.
- Doença rara (ontologia)
- fonte: Orphanet
- Identificador unificado
- fonte: MONDO
- Codificação WHO/SUS
- fonte: WHO ICD-10 / DATASUS
- CID-11 (futuro)
- fonte: WHO ICD-11
- NIH/GARD
- fonte: GARD (NIH)
- Dado público estruturado
- fonte: Wikidata