É um erro genético no metabolismo, presente desde o nascimento. Caracteriza-se pela falta de uma das enzimas (proteínas que ajudam nas reações químicas do corpo) essenciais para o ciclo da ureia. O ciclo da ureia é um processo importante que o corpo usa para eliminar substâncias tóxicas. Como resultado, uma substância chamada amônia se acumula no organismo, o que pode ser prejudicial.
Introdução
O que você precisa saber de cara
É um erro genético no metabolismo, presente desde o nascimento. Caracteriza-se pela falta de uma das enzimas (proteínas que ajudam nas reações químicas do corpo) essenciais para o ciclo da ureia. O ciclo da ureia é um processo importante que o corpo usa para eliminar substâncias tóxicas. Como resultado, uma substância chamada amônia se acumula no organismo, o que pode ser prejudicial.
Encontrou um erro ou informação desatualizada? Sugira uma correção →
Entender a doença
Do básico ao detalhe, leia no seu ritmo
Preparando trilha educativa...
Sinais e sintomas
O que aparece no corpo e com que frequência cada sintoma acontece
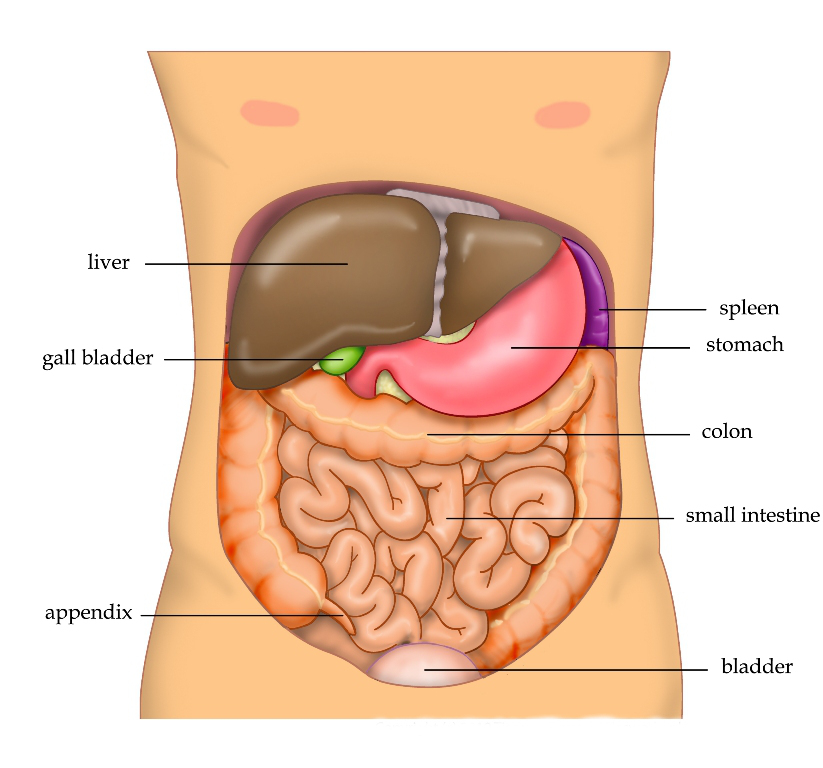
Partes do corpo afetadas
+ 134 sintomas em outras categorias
Características mais comuns
Os sintomas variam de pessoa para pessoa. Abaixo estão as 264 características clínicas mais associadas, ordenadas por frequência.
Linha do tempo da pesquisa
Triagem neonatal (Teste do Pezinho)
A triagem neonatal permite diagnóstico precoce e início imediato do tratamento.
Encontrou um erro ou informação desatualizada? Sugira uma correção →
Genética e causas
O que está alterado no DNA e como passa nas famílias
Genes associados
11 genes identificados com associação a esta condição.
Mitochondrial carbonic anhydrase that catalyzes the reversible conversion of carbon dioxide to bicarbonate/HCO3 (PubMed:24530203, PubMed:8356065). Mitochondria are impermeable to HCO3, and thus this intramitochondrial carbonic anhydrase is pivotal in providing HCO3 for multiple mitochondrial enzymes that catalyze the formation of essential metabolites of intermediary metabolism in the urea and Krebs cycles (PubMed:24530203)
Mitochondrion
Hyperammonemia due to carbonic anhydrase VA deficiency
An autosomal recessive inborn error of metabolism, clinically characterized by infantile hyperammonemic encephalopathy. Metabolic abnormalities include hypoglycemia, hyperlactatemia, metabolic acidosis and respiratory alkalosis.
Catalyzes the reversible cleavage of L-argininosuccinate to fumarate and L-arginine, an intermediate step reaction in the urea cycle mostly providing for hepatic nitrogen detoxification into excretable urea as well as de novo L-arginine synthesis in nonhepatic tissues (PubMed:11747432, PubMed:11747433, PubMed:22081021, PubMed:2263616, PubMed:9045711). Essential regulator of intracellular and extracellular L-arginine pools. As part of citrulline-nitric oxide cycle, forms tissue-specific multiprot
Argininosuccinic aciduria
An autosomal recessive disorder of the urea cycle. The disease is characterized by mental and physical retardation, liver enlargement, skin lesions, dry and brittle hair showing trichorrhexis nodosa microscopically and fluorescing red, convulsions, and episodic unconsciousness.
Biotin-attachment subunit of the 3-methylcrotonyl-CoA carboxylase, an enzyme that catalyzes the conversion of 3-methylcrotonyl-CoA to 3-methylglutaconyl-CoA, a critical step for leucine and isovaleric acid catabolism
Mitochondrion matrix
3-methylcrotonoyl-CoA carboxylase 1 deficiency
An autosomal recessive disorder of leucine catabolism. The phenotype is variable, ranging from neonatal onset with severe neurological involvement to asymptomatic adults. There is a characteristic organic aciduria with massive excretion of 3-hydroxyisovaleric acid and 3-methylcrotonylglycine, usually in combination with a severe secondary carnitine deficiency.
Key element of the urea cycle converting L-arginine to urea and L-ornithine, which is further metabolized into metabolites proline and polyamides that drive collagen synthesis and bioenergetic pathways critical for cell proliferation, respectively; the urea cycle takes place primarily in the liver and, to a lesser extent, in the kidneys Functions in L-arginine homeostasis in nonhepatic tissues characterized by the competition between nitric oxide synthase (NOS) and arginase for the available int
CytoplasmCytoplasmic granule
Argininemia
A rare autosomal recessive disorder of the urea cycle. Arginine is elevated in the blood and cerebrospinal fluid, and periodic hyperammonemia occurs. Clinical manifestations include developmental delay, seizures, intellectual disability, hypotonia, ataxia and progressive spastic quadriplegia.
One of the enzymes of the urea cycle, the metabolic pathway transforming neurotoxic amonia produced by protein catabolism into inocuous urea in the liver of ureotelic animals. Catalyzes the formation of arginosuccinate from aspartate, citrulline and ATP and together with ASL it is responsible for the biosynthesis of arginine in most body tissues
Cytoplasm, cytosol
Citrullinemia 1
The classic form of citrullinemia, an autosomal recessive disease characterized primarily by elevated serum and urine citrulline levels. Ammonia intoxication is another manifestation. It is a disorder of the urea cycle, usually manifesting in the first few days of life. Affected infants appear normal at birth, but as ammonia builds up in the body they present symptoms such as lethargy, poor feeding, vomiting, seizures and loss of consciousness. Less commonly, a milder form can develop later in childhood or adulthood.
Mitochondrial electrogenic aspartate/glutamate antiporter that favors efflux of aspartate and entry of glutamate and proton within the mitochondria as part of the malate-aspartate shuttle (PubMed:11566871, PubMed:38937634, PubMed:38945283, PubMed:39419476). Substrate exchange across the membrane occurs consecutively with one substrate being transported first, then dissociating from the substrate binding site before the second substrate binds for transport in the opposite direction (PubMed:389376
Mitochondrion inner membrane
Citrin deficiency, adolescent or adult onset
An autosomal recessive metabolic disorder characterized by elevated serum and urine citrulline levels, ammonia intoxication, and neuropsychiatric symptoms including abnormal behaviors, loss of memory, seizures and coma. Death can result from brain edema.
Involved in the urea cycle of ureotelic animals where the enzyme plays an important role in removing excess ammonia from the cell
MitochondrionNucleus, nucleolusCell membrane
Carbamoyl phosphate synthetase 1 deficiency
An autosomal recessive disorder of the urea cycle causing hyperammonemia. It can present as a devastating metabolic disease dominated by severe hyperammonemia in neonates or as a more insidious late-onset condition, generally manifesting as life-threatening hyperammonemic crises under catabolic situations. Clinical features include protein intolerance, intermittent ataxia, seizures, lethargy, developmental delay and intellectual disability.
Plays a role in the regulation of ureagenesis by producing the essential cofactor N-acetylglutamate (NAG), thus modulating carbamoylphosphate synthase I (CPS1) activity
Mitochondrion matrix
N-acetylglutamate synthase deficiency
Rare autosomal recessively inherited metabolic disorder leading to severe neonatal or late-onset hyperammonemia without increased excretion of orotic acid. Clinical symptoms are somnolence, tachypnea, feeding difficulties, a severe neurologic presentation characterized by uncontrollable movements, developmental delay, visual impairment, failure to thrive and hyperammonemia precipitated by the introduction of high-protein diet or febrile illness.
Mitochondrial glutamate dehydrogenase that catalyzes the conversion of L-glutamate into alpha-ketoglutarate. Plays a key role in glutamine anaplerosis by producing alpha-ketoglutarate, an important intermediate in the tricarboxylic acid cycle (PubMed:11032875, PubMed:11254391, PubMed:16023112, PubMed:16959573). Plays a role in insulin homeostasis (PubMed:11297618, PubMed:9571255). May be involved in learning and memory reactions by increasing the turnover of the excitatory neurotransmitter gluta
MitochondrionEndoplasmic reticulum
Hyperinsulinemic hypoglycemia, familial, 6
A form of hyperinsulinemic hypoglycemia, a clinically and genetically heterogeneous disorder characterized by inappropriate insulin secretion from the pancreatic beta-cells in the presence of low blood glucose levels. HHF6 is an autosomal dominant form characterized by hypoglycemia due to congenital hyperinsulinism combined with persistent hyperammonemia. Clinical features include loss of consciousness due to hypoglycemia, hypoglycemic seizures, and mental retardation.
Catalyzes the second step of the urea cycle, the condensation of carbamoyl phosphate with L-ornithine to form L-citrulline (PubMed:2556444, PubMed:6372096, PubMed:8112735). The urea cycle ensures the detoxification of ammonia by converting it to urea for excretion (PubMed:2556444)
Mitochondrion matrix
Ornithine carbamoyltransferase deficiency
An X-linked disorder of the urea cycle which causes a form of hyperammonemia. Mutations with no residual enzyme activity are always expressed in hemizygote males by a very severe neonatal hyperammonemic coma that generally proves to be fatal. Heterozygous females are either asymptomatic or express orotic aciduria spontaneously or after protein intake. The disorder is treatable with supplemental dietary arginine and low protein diet. The arbitrary classification of patients into the 'neonatal' group (clinical hyperammonemia in the first few days of life) and 'late' onset (clinical presentation after the neonatal period) has been used to differentiate severe from mild forms.
Mitochondrial ornithine-citrulline antiporter (Probable) (PubMed:12807890, PubMed:22262851). Catalyzes the exchange between cytosolic ornithine and mitochondrial citrulline plus an H(+), the proton compensates the positive charge of ornithine thus leading to an electroneutral transport. Plays a crucial role in the urea cycle, by connecting the cytosolic and the intramitochondrial reactions of the urea cycle (Probable) (PubMed:12807890, PubMed:22262851). Lysine and arginine are also transported b
Mitochondrion inner membraneMitochondrion membrane
Hyperornithinemia-hyperammonemia-homocitrullinuria syndrome
An autosomal recessive disorder of the urea cycle characterized by onset in early life. The acute phase of the disease is characterized by vomiting, ataxia, lethargy, confusion, and coma. Chronic clinical manifestations include hypotonia, developmental delay, progressive encephalopathy with mental regression, and spastic paraparesis with pyramidal signs.
Variantes genéticas (ClinVar)
689 variantes patogênicas registradas no ClinVar.
Vias biológicas (Reactome)
18 vias biológicas associadas aos genes desta condição.
Diagnóstico
Os sinais que médicos procuram e os exames que confirmam
Tratamento e manejo
Remédios, cuidados de apoio e o que precisa acompanhar
Onde tratar no SUS
Hospitais de referência no Brasil e o protocolo oficial do SUS (PCDT)
🇧🇷 Atendimento SUS — Doença do metabolismo do ciclo da ureia e destoxificação da amônia
Centros de Referência SUS
21 centros habilitados pelo SUS para Doença do metabolismo do ciclo da ureia e destoxificação da amônia
Centros para Doença do metabolismo do ciclo da ureia e destoxificação da amônia
Detalhes dos centros
Hospital Universitário Prof. Edgard Santos (HUPES)
R. Dr. Augusto Viana, s/n - Canela, Salvador - BA, 40110-060 · CNES 0003808
Serviço de Referência
Hospital de Apoio de Brasília (HAB)
AENW 3 Lote A Setor Noroeste - Plano Piloto, Brasília - DF, 70684-831 · CNES 0010456
Serviço de Referência
Hospital Estadual Infantil e Maternidade Alzir Bernardino Alves (HIABA)
Av. Min. Salgado Filho, 918 - Soteco, Vila Velha - ES, 29106-010 · CNES 6631207
Serviço de Referência
Hospital das Clínicas da UFG
Rua 235 QD. 68 Lote Área, Nº 285, s/nº - Setor Leste Universitário, Goiânia - GO, 74605-050 · CNES 2338424
Serviço de Referência
Hospital das Clínicas da UFMG
Av. Prof. Alfredo Balena, 110 - Santa Efigênia, Belo Horizonte - MG, 30130-100 · CNES 2280167
Serviço de Referência
NUPAD / Faculdade de Medicina UFMG
Av. Prof. Alfredo Balena, 189 - 5 andar - Centro, Belo Horizonte - MG, 30130-100 · CNES 2183226
Serviço de Referência
Hospital Universitário João de Barros Barreto
R. dos Mundurucus, 4487 - Guamá, Belém - PA, 66073-000 · CNES 2337878
Serviço de Referência
Hospital de Clínicas da Universidade Federal de Pernambuco
Av. Prof. Moraes Rego, 1235 - Cidade Universitária, Recife - PE, 50670-901 · CNES 2561492
Atenção Especializada
Instituto de Medicina Integral Prof. Fernando Figueira (IMIP)
R. dos Coelhos, 300 - Boa Vista, Recife - PE, 50070-902 · CNES 0000647
Serviço de Referência
Hospital de Clínicas da UFPR
R. Gen. Carneiro, 181 - Alto da Glória, Curitiba - PR, 80060-900 · CNES 2364980
Serviço de Referência
Hospital Universitário Pedro Ernesto (HUPE-UERJ)
Blvd. 28 de Setembro, 77 - Vila Isabel, Rio de Janeiro - RJ, 20551-030 · CNES 2280221
Serviço de Referência
Instituto Nacional de Saúde da Mulher, da Criança e do Adolescente Fernandes Figueira (IFF/Fiocruz)
Av. Rui Barbosa, 716 - Flamengo, Rio de Janeiro - RJ, 22250-020 · CNES 2269988
Serviço de Referência
Hospital Universitário Onofre Lopes (HUOL)
Av. Nilo Peçanha, 620 - Petrópolis, Natal - RN, 59012-300 · CNES 2408570
Atenção Especializada
Hospital São Lucas da PUCRS
Av. Ipiranga, 6690 - Jardim Botânico, Porto Alegre - RS, 90610-000 · CNES 2232928
Serviço de Referência
Hospital de Clínicas de Porto Alegre (HCPA)
Rua Ramiro Barcelos, 2350 Bloco A - Av. Protásio Alves, 211 - Bloco B e C - Santa Cecília, Porto Alegre - RS, 90035-903 · CNES 2237601
Serviço de Referência
Hospital Universitário da UFSC (HU-UFSC)
R. Profa. Maria Flora Pausewang - Trindade, Florianópolis - SC, 88036-800 · CNES 2560356
Serviço de Referência
Hospital das Clínicas da FMUSP
R. Dr. Ovídio Pires de Campos, 225 - Cerqueira César, São Paulo - SP, 05403-010 · CNES 2077485
Serviço de Referência
Hospital de Clínicas da UNICAMP
R. Vital Brasil, 251 - Cidade Universitária, Campinas - SP, 13083-888 · CNES 2748223
Serviço de Referência
Hospital de Clínicas de Ribeirão Preto (HCRP-USP)
R. Ten. Catão Roxo, 3900 - Vila Monte Alegre, Ribeirão Preto - SP, 14015-010 · CNES 2082187
Serviço de Referência
Instituto da Criança e do Adolescente (ICr-HCFMUSP)
Av. Dr. Enéas Carvalho de Aguiar, 647 - Cerqueira César, São Paulo - SP, 05403-000 · CNES 2081695
Serviço de Referência
UNIFESP / Hospital São Paulo
R. Napoleão de Barros, 715 - Vila Clementino, São Paulo - SP, 04024-002 · CNES 2688689
Serviço de Referência
Dados de DATASUS/CNES, SBGM, ABNeuro e Ministério da Saúde. Sempre confirme a disponibilidade diretamente com o estabelecimento.
Pesquisa ativa
Ensaios clínicos abertos e novidades científicas recentes
Pesquisa e ensaios clínicos
Nenhum ensaio clínico registrado para esta condição.
Publicações mais relevantes
Nitrogen Scavengers: History, Clinical Considerations and Future Prospects.
Nitrogen scavengers play a critical role in treating acute and chronic hyperammonemia, especially in urea cycle disorders (UCDs), where impaired ammonia detoxification leads to toxic nitrogen accumulation. These agents complement low-protein diets and urea cycle intermediates. Sodium benzoate and sodium phenylacetate are the main scavengers, conjugating with glycine and glutamine to form hippurate and phenylacetylglutamine, which are excreted in urine. This therapeutic approach, introduced in the 1980s, was based on early findings linking benzoate to reduced urea excretion. Nitrogen scavengers are also used in secondary hyperammonemia from organic acidemias and fatty acid oxidation disorders, though they may become increasingly ineffective in progressing liver failure due to their reliance on hepatocyte function. To improve tolerability, phenylbutyrate was developed as an oral alternative to phenylacetate and is available in sodium-bound and prodrug forms, but issues with taste and side effects persist. While effective, current treatments target nitrogenous waste products rather than ammonia directly, offering an avenue of future drug development for UCDs. This review discusses the chemical properties, clinical use, and limitations of nitrogen scavengers, hereby focusing on phenylacetate and related substances, and highlights the need for improved therapies, including approaches that directly target ammonia removal. For the benefit of readers already experienced in nitrogen scavengers for UCDs, we also include considerations concerning the use of these drugs in animal experiments and a viewpoint on ornithine phenylacetate as a related substance.
The Current Status of Adult Patients With Urea Cycle Disorders in Japan: From the Nation-Wide Study.
Urea cycle disorders (UCDs) are rare inherited metabolic diseases characterized by defective detoxification of nitrogen, leading to hyperammonemia and neurological complications. While pediatric UCDs have been extensively studied in Japan, data on adult patients remain limited. This study aims to evaluate the current status of Japanese adult UCD patients, hereby comparing long-term outcomes after neonatal/infantile or late onset in a new nationwide study investigating clinical manifestations and management. In total, we collected data of 116 adult UCD patients diagnosed and/or treated at various institutions, combining this new cohort (34 UCD patients between January 2010 and December 2022) with data from a previous nationwide study (82 UCD patients between January 2000 and March 2018). Among 116 adult UCD patients, ornithine transcarbamylase deficiency was the most common subtype (N = 69). Hyperammonemia occurred in 91.4% of patients, and intellectual disability was present in 50.0%. Patients generally showed reduced final height and BMI compared to Japanese controls, particularly among females and those with infantile-onset UCDs. Peak ammonia levels ≥ 360 μmol/L were significantly associated with intellectual disability. Liver transplantation (LT) was performed in 20 patients, and although it helped to avoid hyperammonemia, it did not statistically improve neurocognitive outcomes in patients with peak ammonia < 360 μmol/L. This study provides the first comprehensive overview of adult UCD patients in Japan, highlighting frequent growth impairment and variable cognitive outcomes. LT improves metabolic control but cannot prevent intellectual disability in all patients. These findings underscore the need for early diagnosis, individualized treatment strategies, and long-term follow-up into adulthood.
Hyperammonemia in urea cycle disorders: A toxic metabolite for the brain.
Ammonia can easily cross the blood-brain barrier in its non-ionized form, leading to significant accumulation in the brain during severe hyperammonemia. Excess ammonia is highly toxic to the brain and can cause neurological dysfunctions, such as tremors, ataxia, seizures, coma, and even death. Hyperammonemia is often the primary manifestation of urea cycle disorders (UCDs), a group of inherited metabolic disorders characterized by impaired nitrogen detoxification due to dysfunctions in urea cycle-related enzymes and transporters. Patients with complete deficiencies of urea cycle enzymes typically present with lethargy, hypothermia, anorexia, seizures, abnormal respiratory patterns (hyperventilation or hypoventilation), neurologic posturing, and coma, along with hyperammonemia within a few days after birth. This condition, classified as the neonatal-onset type, frequently results in severe hyperammonemic encephalopathy (≥600 μg/dL [360 μmol/L]) at onset. Hyperammonemia with blood ammonia levels of 600 μg/dL (360 μmol/L) or higher causes significant brain damage. Therefore, at this threshold, hemodialysis is indicated to rapidly remove ammonia and mitigate its harmful effects on the brain. However, even when neonatal-onset UCD patients undergo a combination of hemodialysis and liver transplantation at the onset of severe hyperammonemia (≥600 μg/dL [360 μmol/L]), the neuroprotective effects remain limited. This review aims to describe the pathophysiology of hyperammonemia and UCDs, the impact of hyperammonemia on the brain in UCDs, the role of current therapeutic strategies, and the challenges associated with future treatments for UCDs.
Novel Treatment Strategy for Patients With Urea Cycle Disorders: Pharmacological Chaperones Enhance Enzyme Stability and Activity in Patient-Derived Liver Disease Models.
Urea cycle disorders (UCDs) are inherited diseases causing recurrent life-threatening metabolic decompensations due to impaired hepatic ammonia detoxification and decreased ureagenesis. Ornithine transcarbamylase (OTC) deficiency (OTCD) is X-linked and the most common and often fatal UCD. In male hemizygous patients, disease severity primarily depends on the pathogenic sequence variant, while in heterozygous females, disease severity also depends on the X-chromosomal inactivation (XCI) pattern. Females with unfavorable XCI predominantly expressing the mutant OTC protein may be severely affected. Here, we investigated a novel treatment strategy for OTCD since there is an unmet need for better therapies. In the first step, we performed a high throughput screening (HTS) using a diversity library with 10 000 chemical compounds to identify pharmacological chaperone (PC) candidates that stabilize purified wild-type OTC. Stratification of our HTS results revealed five potential PCs, which were selected for further experimentation in cellular systems using primary human hepatocytes (PHHs) and human induced pluripotent stem cell (hiPSC)-derived hepatocytes (hiPSC-Heps) from healthy controls and OTCD patients. Two PCs-PC1 and PC4-increased OTC protein stability and activity in control hiPSC-Heps, while PC4 in addition increased OTC activity in patient-derived PHHs from a female OTCD patient with unfavorable XCI. Finally, PC1 and PC4 both significantly increased ureagenesis in patient-derived PHHs. To conclude, we identified two PCs that stabilized wild-type OTC and enhanced enzyme activity and ureagenesis. Our work suggests that PCs could provide a novel treatment strategy for OTCD specifically in females with unfavorable XCI.
Radiation therapy in a ductal carcinoma in situ patient with ornithine transcarbamylase deficiency: a case report.
Ornithine transcarbamylase (OTC) deficiency is a rare urea cycle disorder that impairs ammonia detoxification, increasing the risk of hyperammonemic crises under metabolic stress. While chemotherapy-related risks have been reported, data on the safety of ionizing radiation therapy (RT) in this population are limited. This case describes a 30-year-old woman with late-onset OTC deficiency diagnosed with right-sided ductal carcinoma in situ. She underwent segmental mastectomy followed by adjuvant 3D conformal RT (40 Gy in 15 fractions with a concomitant boost to 48 Gy). Her multidisciplinary care involved preoperative hydration, close nutritional monitoring, and serial ammonia measurements. She completed RT without treatment interruptions or signs of hyperammonemia. This case illustrates that breast RT can be delivered safely in patients with OTC deficiency with a multidisciplinary, preventative approach. To our knowledge, this is the first report describing RT planning and metabolic surveillance in this population.
Publicações recentes
[A 71-year-old woman with adult-onset type II citrullinemia, initially presenting with normal blood ammonia levels].
[Hyperammonemia and metabolic-associated fatty liver disease: a complex relationship].
Nitrogen Scavengers: History, Clinical Considerations and Future Prospects.
[Clinical characteristics and efficacy of glyceryl phenylbutyrate treatment in 20 pediatric patients with urea cycle disorder].
Hyperammonemia in urea cycle disorders: A toxic metabolite for the brain.
📚 EuropePMCmostrando 33
Radiation therapy in a ductal carcinoma in situ patient with ornithine transcarbamylase deficiency: a case report.
Radiation oncology journalHyperuricemia increases susceptibility to chronic kidney injury exacerbation via autophagic flux blockade-mediated ammonia death pathway.
Journal of advanced researchNitrogen Scavengers: History, Clinical Considerations and Future Prospects.
Journal of inherited metabolic diseaseThe Current Status of Adult Patients With Urea Cycle Disorders in Japan: From the Nation-Wide Study.
Journal of inherited metabolic diseaseCurrent Treatment Modalities for Urea Cycle Disorders.
Paediatric drugsAmino Acid Metabolism in Liver Mitochondria: From Homeostasis to Disease.
MetabolitesHyperammonemia in urea cycle disorders: A toxic metabolite for the brain.
Pediatrics international : official journal of the Japan Pediatric SocietyNovel Treatment Strategy for Patients With Urea Cycle Disorders: Pharmacological Chaperones Enhance Enzyme Stability and Activity in Patient-Derived Liver Disease Models.
Journal of inherited metabolic diseaseA novel de novo missense OTC mutation in an Iranian girl: a case report.
Journal of pediatric endocrinology & metabolism : JPEMQuo vadis ureagenesis disorders? A journey from 90 years ago into the future.
Journal of inherited metabolic diseaseChallenges of managing ornithine transcarbamylase deficiency in female heterozygotes.
Molecular genetics and metabolism reportsSafety and efficacy of an engineered hepatotropic AAV gene therapy for ornithine transcarbamylase deficiency in cynomolgus monkeys.
Molecular therapy. Methods & clinical development[Aciduria argininosuccínica: informe de un caso de inicio neonatal].
Archivos argentinos de pediatriaLong-term outcome of urea cycle disorders: Report from a nationwide study in Japan.
Journal of inherited metabolic diseasePrimary hyperammonaemia: Current diagnostic and therapeutic strategies.
Journal of mother and childMetabolic basis and treatment of citrin deficiency.
Journal of inherited metabolic diseaseTherapeutic effect of N-carbamylglutamate in CPS1 deficiency.
Molecular genetics and metabolism reportsUsefulness of Carnitine Supplementation for the Complications of Liver Cirrhosis.
NutrientsAmmonia uptake by transmembrane pH gradient poly(isoprene)-block-poly(ethylene glycol) polymersomes.
Soft matterInborn errors of enzymes in glutamate metabolism.
Journal of inherited metabolic diseaseSimultaneous quantification of 48 plasma amino acids by liquid chromatography-tandem mass spectrometry to investigate urea cycle disorders.
Clinica chimica acta; international journal of clinical chemistryChallenges in diagnosing and managing adult patients with urea cycle disorders.
Journal of inherited metabolic diseaseMalnutrition with hypoaminoacidemia in a 22-year-old pregnant patient masking a likely ornithine transcarbamylase deficiency.
Clinical nutrition ESPENHepatic glutamine synthetase augmentation enhances ammonia detoxification.
Journal of inherited metabolic diseaseComprehensive characterization of ureagenesis in the spfash mouse, a model of human ornithine transcarbamylase deficiency, reveals age-dependency of ammonia detoxification.
Journal of inherited metabolic diseaseAmmonia and autophagy: An emerging relationship with implications for disorders with hyperammonemia.
Journal of inherited metabolic diseaseMedium-chain triglycerides supplement therapy with a low-carbohydrate formula can supply energy and enhance ammonia detoxification in the hepatocytes of patients with adult-onset type II citrullinemia.
Journal of inherited metabolic diseaseVariable X-chromosome inactivation and enlargement of pericentral glutamine synthetase zones in the liver of heterozygous females with OTC deficiency.
Virchows Archiv : an international journal of pathologyEnhancement of hepatic autophagy increases ureagenesis and protects against hyperammonemia.
Proceedings of the National Academy of Sciences of the United States of AmericaClinical course of 63 patients with neonatal onset urea cycle disorders in the years 2001-2013.
Orphanet journal of rare diseasesIn vivo monitoring of urea cycle activity with (13)C-acetate as a tracer of ureagenesis.
Molecular genetics and metabolismStructure of human carbamoyl phosphate synthetase: deciphering the on/off switch of human ureagenesis.
Scientific reportsRecent advances in the treatment of hyperammonemia.
Advanced drug delivery reviewsAssociações
Organizações que acompanham esta doença — pra ter apoio e orientação
Ainda não temos associações cadastradas para Doença do metabolismo do ciclo da ureia e destoxificação da amônia.
É de uma associação que acompanha esta doença? Fale com a gente →
Comunidades
Grupos ativos de quem convive com esta doença aqui no Raras
Ainda não existe comunidade no Raras para Doença do metabolismo do ciclo da ureia e destoxificação da amônia
Pacientes, familiares e cuidadores se organizam em comunidades pra compartilhar experiências, fazer perguntas e se apoiar. Você pode ser o primeiro.
Tire suas dúvidas
Perguntas, dicas e experiências compartilhadas aqui na página
Participe da discussão
Faça login para postar dúvidas, compartilhar experiências e interagir com especialistas.
Fazer loginDoenças relacionadas
Doenças com sintomas parecidos — ajudam quem ainda está buscando diagnóstico
Referências e fontes
Bases de dados externas citadas neste artigo
Publicações científicas
Artigos indexados no PubMed ligados a esta doença no grafo RarasNet — título, periódico e PMID direto da fonte, sem intermediação de IA.
- Nitrogen Scavengers: History, Clinical Considerations and Future Prospects.
- The Current Status of Adult Patients With Urea Cycle Disorders in Japan: From the Nation-Wide Study.
- Hyperammonemia in urea cycle disorders: A toxic metabolite for the brain.Pediatrics international : official journal of the Japan Pediatric Society· 2025· PMID 40464331mais citado
- Novel Treatment Strategy for Patients With Urea Cycle Disorders: Pharmacological Chaperones Enhance Enzyme Stability and Activity in Patient-Derived Liver Disease Models.
- Radiation therapy in a ductal carcinoma in situ patient with ornithine transcarbamylase deficiency: a case report.
- [A 71-year-old woman with adult-onset type II citrullinemia, initially presenting with normal blood ammonia levels].
- [Hyperammonemia and metabolic-associated fatty liver disease: a complex relationship].
- [Clinical characteristics and efficacy of glyceryl phenylbutyrate treatment in 20 pediatric patients with urea cycle disorder].
Bases de dados e fontes oficiais
Identificadores e referências canônicas usadas para montar este verbete.
- ORPHA:79167(Orphanet)
- MONDO:0004739(MONDO)
- GARD:7837(GARD (NIH))
- Variantes catalogadas(ClinVar)
- Busca completa no PubMed(PubMed)
- Q1585743(Wikidata)
Dados compilados pelo RarasNet a partir de fontes abertas (Orphanet, OMIM, MONDO, PubMed/EuropePMC, ClinicalTrials.gov, DATASUS, PCDT/MS). Este conteúdo é informativo e não substitui avaliação médica.
Conteúdo mantido por Agente Raras · Médicos e pesquisadores podem colaborar
Doença do metabolismo do ciclo da ureia e destoxificação da amônia
📋 Origem dos dados
Esta página agrega dados de fontes públicas e oficiais. Dados sobre cobertura no SUS (PCDT, CEAF) são verificados ativamente por agente proativo (ver badge no infobox). Demais dados têm atribuição de fonte + data da última sincronização — clique para abrir o original.
- Doença rara (ontologia)
- fonte: Orphanet
- Identificador unificado
- fonte: MONDO
- Codificação WHO/SUS
- fonte: WHO ICD-10 / DATASUS
- NIH/GARD
- fonte: GARD (NIH)
- Indexação biomédica
- fonte: MeSH (NLM)
- Dado público estruturado
- fonte: Wikidata